







Retina practices sit in an unusual position in medicine. We routinely stock and administer some of the most expensive drugs in outpatient care—anti-VEGF agents, corticosteroid implants, and complement inhibitors—at volumes that dwarf all other financial sectors of our practices. A busy retina doctor might push through dozens of injections a day, each involving a drug costing thousands of dollars per dose. Multiply that across hundreds of doses per month, and you’re managing inventory that represents the vast majority of your financial throughput, dwarfing other revenue streams and working capital alike. The exposure only multiplies with multiple doctors.
Yet, the way many practices manage that inventory hasn’t kept pace with the financial stakes. Some of the sharpest clinical minds in ophthalmology are still tracking 6-figure monthly drug spends on spreadsheets—or worse, on paper logs taped to the refrigerator door.
Here, I present a case for making the jump to an inventory management system. If your practice is still on spreadsheets, the things you’re sacrificing most are accuracy and speed—and in a specialty where a single billing error or expired vial can cost thousands of dollars (a full day’s or week’s profit for a given doctor), those aren’t abstractions. Below, we look at the current landscape of inventory tools, how they differ, what electronic health record (EHR) integration actually means in operational terms, and why the gap between a dedicated system and a spreadsheet shows up directly on your bottom line.
The Spreadsheet Reality
A meaningful number of retina practices (including some large ones) still manage drug inventory on Excel or Google Sheets. In some cases, the spreadsheet is surprisingly sophisticated, with formulas tracking lot numbers, expiration dates, and reorder points. In most cases, it’s not.
The appeal is obvious. Spreadsheets are free, every staff member knows how to use one, and there’s no implementation process or vendor contract. For a small practice doing modest injection volume, a well-maintained spreadsheet can technically get the job done.
If your practice is still on spreadsheets, the things you’re sacrificing most are accuracy and speed—and in a specialty where a single billing error or expired vial can cost thousands of dollars, those aren’t abstractions.
The problems emerge at scale, and they emerge quietly. A spreadsheet doesn’t alert you when a vial is approaching expiration or when a number has been keyed incorrectly. It can’t reconcile what was dispensed against what was billed in real time. And it cannot tell you whether the vial billed to a patient's insurance was actually the one drawn up and injected—or, for that matter, whether the eye billed matches the eye injected.
The cost of these gaps is hard to quantify because it’s distributed across many smaller losses: an expired vial here, a billing discrepancy there, staff time on manual counts. These are often less visible to practice owners and simply thought of as part of the job by staff. But practices that have transitioned to dedicated inventory systems consistently report aggregate savings—reduced waste, improved billing accuracy, recovered staff hours—that more than justify the cost of the system. The question is usually not whether the practice was losing money on manual tracking, but how much.
Medication Inventory Systems: What to Look For
Several inventory management platforms have been developed specifically for retina practices, or at least with retina workflows as a primary use case. They differ meaningfully in technology, business models, and integration capabilities.
The Integration Question: Unidirectional vs. Bidirectional
To me, this is the single most important aspect of your inventory system and what should ultimately drive your choice—not to mention where the true value inflection point lies. Many practices may be making decisions without fully understanding what they’re choosing between.
When an inventory system integrates with your EHR, that integration can work in 1 of 2 ways. Understanding the difference matters dramatically:
-
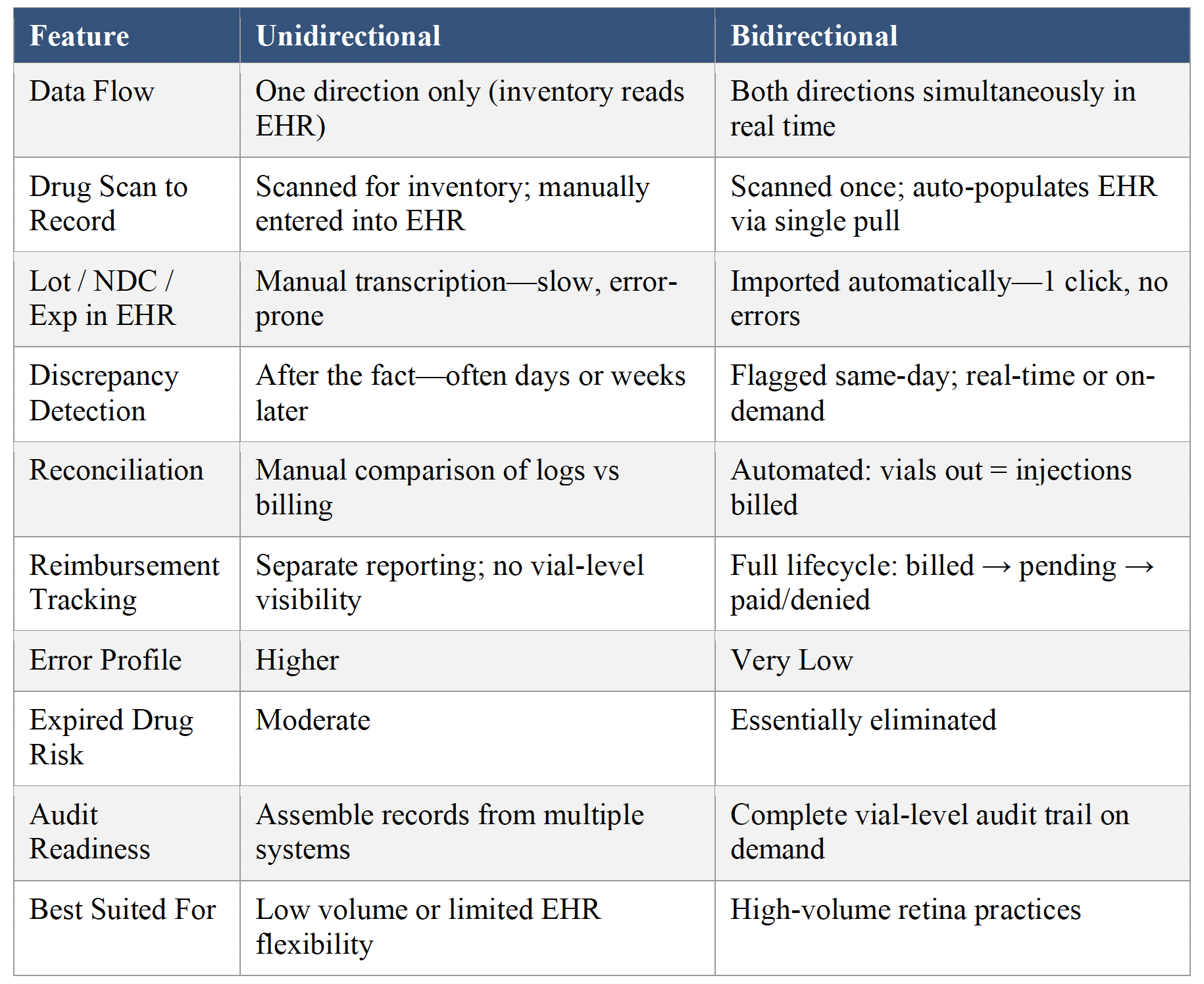
Unidirectional integration means data flows in 1 direction—typically from the EHR to the inventory system, but not back. The inventory system reads from the EHR but does not write to it.
-
Bidirectional integration means data flows both ways in real time, creating a closed-loop workflow that meaningfully changes how your team handles injections. The inventory system reads from your EHR and writes back to it.
Here’s what that looks like in practice, when ideally implemented:
-
A drug shipment arrives. Meds are unboxed, visually counted, and received in the inventory system with 1 click for the whole shipment (preloaded into the system).
-
Upon administration, the tech removes the drug from the refrigerator and scans and dispenses that dose (to the correct patient and eye), with patient and encounter details automatically pre-loaded from the EHR.
-
The physician administers the medication.
-
The scribe or injection tech clicks the “pull” button in the EHR procedure note, and the lot number, expiration date, and National Drug Code (NDC) are automatically imported (and in some cases billing modifiers are updated).
It is that last step that separates bidirectional from everything else: a single pull that imports compliance-critical data directly from the inventory system into the patient’s medical record. No transcription. No handwritten lot numbers. No technician squinting at a vial label. The information that has to be right for billing, documentation, and any future audit arrives with 100% accuracy because it was never manually entered. Dose receiving, dose administration, and medical record keeping all carry that same accuracy.
At the end of the day, or on demand, staff run a reconciliation check: Does the number of vials reduced from inventory match the number of injections billed? If something doesn’t line up—a wasted vial not documented, an incorrect or missing billing code or laterality, a cancelled injection—the system flags it immediately. You’re catching discrepancies the same day, when staff still has a of the clinical session.
Beyond daily reconciliation, a bidirectional system gives you visibility into where each dose sits in the reimbursement pipeline. Was it billed? Paid? Pending prior auth? Sitting in a denial queue? For me, the inventory management system gives a much clearer view of medication dose revenue cycle than my EHR alone.
Compare that to a unidirectional setup where staff manually enters lot numbers, separately reconciles dispensing logs against billing reports, and chases down discrepancies after the fact. The difference isn’t incremental. It’s dramatic. I believe that if you are evaluating inventory management systems, bidirectional EHR integration should be a requirement. This distinction is much more important than which specific system you choose.
Receiving and Scanning
I have found it a dramatic savings in staff time to have incoming shipments preloaded in the system. When a delivery arrives, receiving staff does a quick visual count to confirm it matches the order, puts doses in the refrigerator, and clicks 1 button in the inventory system to acknowledge receipt—automatically loading every vial with its lot number, NDC, and expiration. No individual scanning. I highly suggest avoiding systems that require scanning every dose at receiving. An exception may be compounded bevacizumab, but it is possible to find vendors that offer bevacizumab pre-labeled and pre-loaded into your system.
Another point: I see clinics installing scanners in every exam room. This is an option but unnecessary—a simpler solution is 1 scanner at the clinic refrigerator, where the drug is scanned as it’s pulled and taken to the patient room.
I often hear concerns about the time and effort of implementation. Having worked closely with implementing 2 separate inventory systems in my practice, I can say implementation has essentially no impact on clinical speed or volume. There is some staff time for coordination and training, but it’s not exorbitant. Making the switch is really about willingness.
The Distributor-Tied Model: Free vs Flexible
Some inventory systems are offered at no direct cost, with a condition: you purchase drugs through a specific distributor. This is the model behind PODIS (Besse Medical, part of Cencora), for example. For many practices, the trade-off is perfectly acceptable—a functional tool without a monthly check. But tying your system to a single distributor narrows purchasing flexibility. If another wholesaler offers better pricing, or supply chain disruptions affect your distributor’s stock, you’re more constrained.
Systems like ArbiMed (Elevate Health Technologies) and RetinaOS (McKesson) take a different approach—distributor-agnostic, working regardless of where you buy, but potentially carrying a monthly cost.
The truth is that most systems are similar in critical operational features (scanning, reporting, error detection), but each one may integrate with your specific EHR unidirectionally or bidirectionally. The differences mostly come down to integration depth and whether you’re willing to tie purchasing to a specific distributor in exchange for a free system. While you can’t always have your first choice on both, these are the key factors.
A Regulatory Note: The DSCSA Exemption
A question that comes up periodically is: Do retina practices need to comply with the Drug Supply Chain Security Act (DSCSA) chain-of-custody tracking requirements? No. We buy-and-bill drugs and administer them in the office as part of our normal practice pattern—the DSCSA explicitly exempts licensed practitioners in that role. But that exemption isn’t an excuse for loose inventory practices. The reasons to track your drug inventory tightly have nothing to do with DSCSA compliance. They have everything to do with running a solvent practice and the legal and compliance issues with medical record-keeping.
The Bottom Line
The core argument is simple: accuracy and speed. A dedicated inventory system gives you both. Spreadsheets give you neither—not reliably, not at scale. A single episode of imprecise inventory management (such as unreported waste, missed billings, expired product, or staff hours burned on manual reconciliation) can easily cost more than an entire year of subscription fees for a dedicated system. The math is not close.
If you’re still on spreadsheets, the first step is acknowledging that what feels like it’s working may actually be costing you money in ways you can’t see. If you’re already using an inventory system, the question worth asking is whether your current integration is truly bidirectional.
The technology exists to make drug inventory management a closed-loop process: received, stored, scanned to patient, documented in the EHR with a single pull, billed, reconciled, and tracked through reimbursement—without manual handoffs at any step. In my opinion, the benefits of these systems dramatically outweigh the costs when considered comprehensively. OM
