







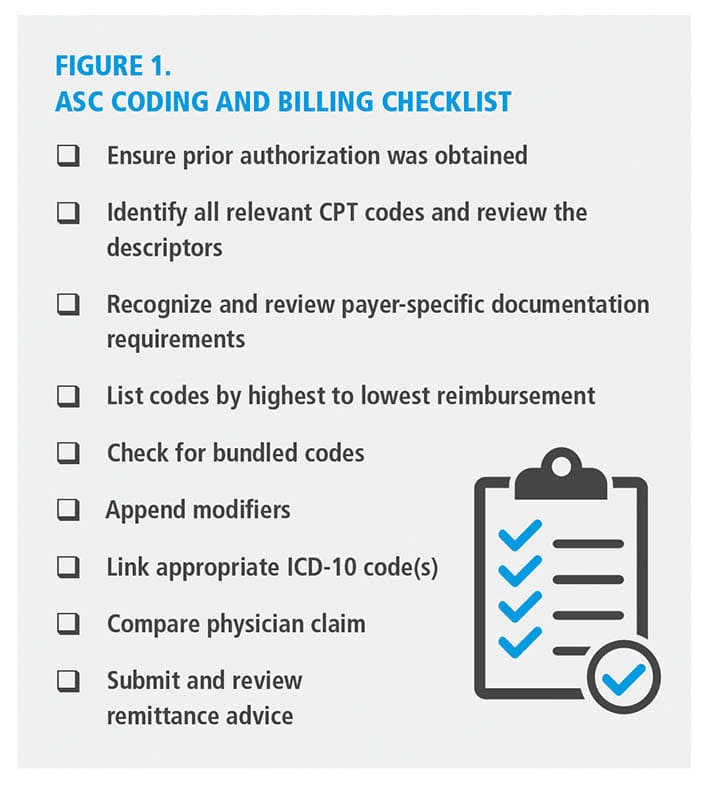
Published in February 2024, the ASC Coding and Billing Checklist* offers a comprehensive, step-by-step framework designed to assist ambulatory surgery centers (ASCs) in managing the complexities of surgical coding and billing (Figure 1). This checklist introduced a structured approach to support coding accuracy, ensure payer compliance, and secure appropriate reimbursement.
This follow-up article builds on that foundation by applying the checklist to two additional surgical scenarios. These examples further demonstrate how to utilize the checklist effectively, whether dealing with standard or complex cataract procedures or advanced retinal repairs. The goal remains to improve coding accuracy and minimize incorrect reimbursement-related issues.
Case Example #1:
Vitrectomy for Macular Hole Repair
Diagnosis
In this case, the diagnosis was a macular hole in the right eye.
Procedures Performed
The procedures included a pars plana vitrectomy (PPV), macular hole repair with internal limiting membrane (ILM) peel, endolaser photocoagulation, and injection of 16% C3F8 gas. A crucial step in surgical coding is verifying that the procedures listed match the description in the body of the operative report. In these cases, consistency is presumed.
Prior Authorization
Vitrectomy and gas injection are often subject to prior authorization by commercial payers. Be sure to always obtain prior authorization for all potential procedure codes. There’s
no downside to authorizing codes that aren’t ultimately used—but failing to get required authorization can result in denied reimbursement.
Code Identification, Review,and Bundling Edits
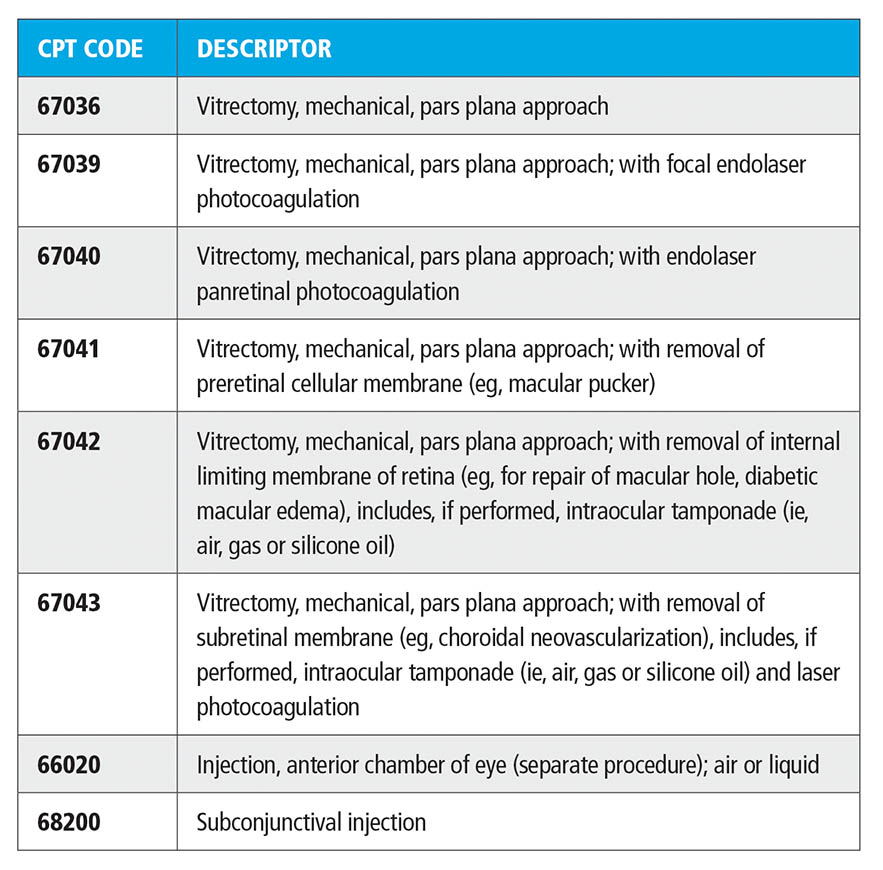
Possible CPT codes based on the description include those found in the table below.
After comparing the operative details to the code descriptors, it was found that certain codes were more appropriate for capturing the full scope of the procedure. Codes such as 67036, 67040,67041 were either more limited or redundant, while CPT 66020 and 68200 were bundled and not separately billable. Further analysis was needed to determine
the most accurate code for the procedure.
Final Code Selection
Both CPT 67039 and 67042 match the description for the procedure, but CPT 67042 is the better choice as the two codes are bundled and have higher RVUs.
Documentation Requirements
The operative report must clearly document the use of ICG dye,
the ILM peel, air-fluid exchange,
and the placement of C3F8 gas
if performed in addition to a valid, covered diagnosis.
Code Order and Modifiers
Only one primary CPT code, 67042, is used, with modifier -RT to denote the right eye. The correct ICD-10 diagnosis is H35.341, indicating a macular hole in the right eye. Check that physician and facility coding align to ensure claim accuracy.
Case Example #2: Intraocular Lens Exchange Wth Scleral Fixation
Diagnosis
The diagnosis for this case was a dislocated intraocular lens (IOL) in the left eye.
Procedures Performed
The surgical interventions included IOL exchange with 27-gauge scleral fixation, pars plana vitrectomy, and subconjunctival injections. Once again, it is crucial to verify that the procedures listed and the descriptions in the operative report are consistent.
Prior Authorization
Identify the payor and confirm whether prior authorization is required. If prior authorization is necessary and not obtained, payment will be denied.
Code Identification, Review, and Bundling Edits
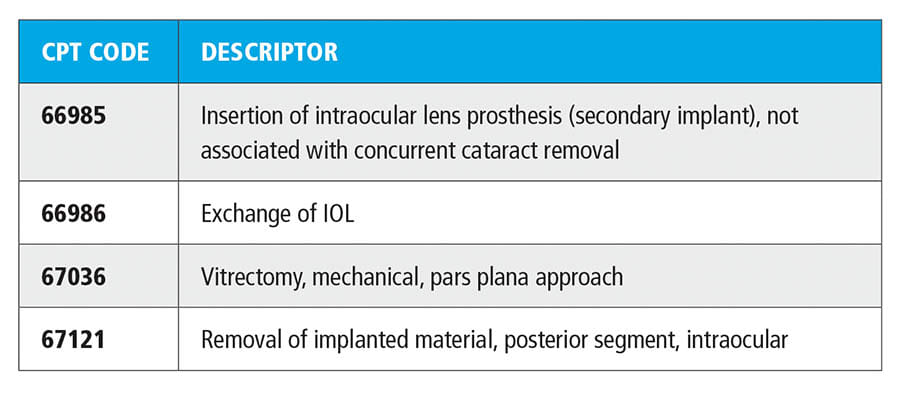
Possible CPT codes based on this scenario’s description include those listed in the table above.
When reviewing the possible CPT codes and their descriptions, CPT 66985 can be excluded as it pertains to secondary IOL implantation without removal of the existing lens. CPT 67121 did not apply, as the IOL was removed from the anterior segment rather than the posterior segment. Further review was needed to determine the most accurate code for the lens exchange.
Final Code Selection
The final code selection includes 2 CPT codes; 66986 for the IOL exchange and 67036 for the vitrectomy. These 2 codes are not bundled (67121 and 67036 are).
Documentation Requirements
Documentation must clearly state that the IOL was dislocated and required removal and must justify the vitrectomy with a covered diagnosis as required by the payor.
Code Order and Modifiers
The code order should list 66986 first, followed by 67036 (66986 has the higher RVUs). No modifier is needed to unbundle these procedures as they are not bundled per NCCI edits. Modifier -LT should be applied to both codes to indicate the procedure was performed on the left eye.
ICD-10 Coding and Physician Alignment
The ICD-10 codes for this case include H43.392 (other vitreous opacities, left eye) for the vitrectomy and T85.22XA (displacement of intraocular lens, initial encounter) for the exchange of IOL. It is essential that the physician’s CPT and ICD-10 coding match the facility’s to maintain claim integrity.
The ICD-10 codes for this case include H43.392 (other vitreous opacities, left eye) for the vitrectomy and T85.22XA (displacement of intraocular lens, initial encounter) for the exchange of IOL. It is essential that the physician’s CPT and ICD-10 coding match the facility’s to maintain claim integrity.
Final Checklist Steps for All Cases
Modifier Use
Always apply appropriate laterality modifiers -RT or -LT or -50 for bilateral per payer guidelines.
ICD-10 Linking
Each CPT code must be clearly supported by a medically necessary ICD-10 diagnosis to support the procedure.
Compare Physician Claims
Ensure that coding for the physician claim and the ASC claim is consistent.
The investment in time is worthwhile, as misalignment can lead to denials, audits, or claim rejections.
Review Remittance Advice
After payment, review remittance advice to confirm that reimbursement matches submitted claims. Appeal any discrepancies promptly.
Consistency is Key
By working through each step of the ASC Coding and Billing Checklist, coders can avoid denials, maintain payer compliance, and optimize reimbursement. For managing everything from cataract-glaucoma combination cases to trauma-related surgeries, consistent adherence to documentation and billing standards is critical for successful claims processing. OASC
Reference
- Baugh M. ASC Coding and Billing Checklist. Ophthalmology Management. Accessed April 29, 2025. https://ophthalmologymanagement.com/supplements/2024/the-ophthalmic-asc-february/coding-and-compliance-asc-coding-and-billing-checklist/
