







For decades, management of keratoconus (KCN) and other irregular-cornea conditions has followed a familiar path from glasses, to rigid or scleral contact lenses, to, ultimately, corneal transplantation when more conservative measures fail. While effective, this pathway leaves many patients in a prolonged gray zone: struggling with vision and contact lens tolerance, but not yet candidates for keratoplasty.
Intracorneal ring segments (ICRS) were introduced in the early 2000s to fill this gap by mechanically reshaping the cornea from within. In selected patients, ICRS could flatten the cornea and improve functional vision. However, early enthusiasm was limited by 2 major issues:
-
ICRS did not address the underlying biomechanical instability of keratoconus, and therefore did not halt disease progression.
-
Outcomes were variable, with ongoing concerns about migration, extrusion, glare, and higher-order aberrations.
Interest in ICRS was reignited in 2016, when corneal cross-linking (CXL) became available in the United States, allowing surgeons to combine a “flattening” procedure (ICRS) with a “freezing” procedure (CXL). Even with this combined approach, however, issues with refractive predictability and implant-related complications persisted, limiting broader adoption. As of publication, the only USFDA-approved intracorneal segments are INTACS, manufactured by Addition Technology, Inc.
Today, newer tissue-based intrastromal reshaping procedures, commonly referred to as CAIRS (corneal allogenic intrastromal ring segments) and CTAK (corneal tissue addition keratoplasty), represent an evolution of the ICRS concept: replacing synthetic implants with donor corneal tissue, then reshaping the cornea by adding tissue rather than removing it. These procedures offer a practical opportunity to expand care options for patients with irregular corneas while integrating well into modern anterior segment and refractive practices.
From Synthetic Rings to Biologic Tissue: Why the Shift?
Traditional ICRS shorten the corneal arc length by inserting rigid polymethylmethacrylate (PMMA) segments into mid-stromal channels. While effective in some cases, several factors limited broader use:
-
Variable refractive predictability, especially in asymmetric or advanced KCN
-
Mechanical complications, such as migration and extrusion
-
Visual symptoms from peripheral optical zone effects
-
Limited customization based on fixed segment geometries
-
Inconsistent device availability in recent years
These limitations helped drive interest in reshaping approaches that preserve the biomechanical concept of ICRS while improving biocompatibility, customization, and (potentially) long-term tolerance. This is where tissue-addition techniques came into play.
Tissue-Based Intrastromal Corneal Reshaping: CAIRS and CTAK
Rather than viewing CAIRS and CTAK as entirely separate procedures, it is helpful to think of them as 2 variations of the same biologic reshaping strategy: implanting donor stromal tissue into intrastromal channels to flatten and regularize the cornea. For patients, both can be described simply as using donor corneal tissue to reshape the cornea from within.
In both approaches, tunnels (either manually created or generated with a femtosecond laser) are placed in the mid-to-deep peripheral cornea, outside the visual axis. Crescent-shaped donor stromal segments are inserted, producing:
-
Central corneal flattening
-
Reduced asymmetry
-
Improved surface regularity
Clinically, this can translate to:
-
Improved uncorrected visual acuity (UCVA)
-
Improved spectacle-corrected visual acuity (BCVA)
-
Improved contact lens-corrected acuity and tolerance
-
Delayed or avoided keratoplasty in selected patients
Because no corneal tissue is removed and the optical zone is preserved, future options for keratoplasty remain available if disease progresses.
Historically, clinicians often accepted poor uncorrected and spectacle vision in KCN patients on the assumption that “a contact lens will fix it.” While rigid and scleral lenses can provide excellent optics, this does not reflect real-world experience. Many patients cannot wear lenses comfortably all day. They struggle during allergy season or ocular surface flares, and face practical challenges with travel, work, and sports. Even modest improvements in uncorrected or glasses-corrected vision can meaningfully reduce dependence on contact lenses and improve daily function. In this context, tissue-based reshaping should be viewed not only as a way to improve lens fit, but also as a strategy to enhance baseline visual function across multiple correction states.
Same Goal, Different Preparation
In CAIRS, the surgeon manually dissects donor corneal tissue into stromal segments. While this can lower material costs, it creates greater variability in segment geometry, less precise customization, and added surgical preparation and technical demands.
Soosan Jacob, MD, deserves recognition for advancing our understanding of CAIRS. In her early cohorts, patients demonstrated clinically significant improvements in UCVA, BCVA, keratometry values, and corneal asphericity.1
For CTAK—introduced in 2016 by Peter Hersh, MD, Steven Gelles, MD, and Steven Greenstein, MD—eye banks use a femtosecond laser to cut gamma-irradiated donor tissue, guided by preoperative tomography and planning protocols (Figure 1).

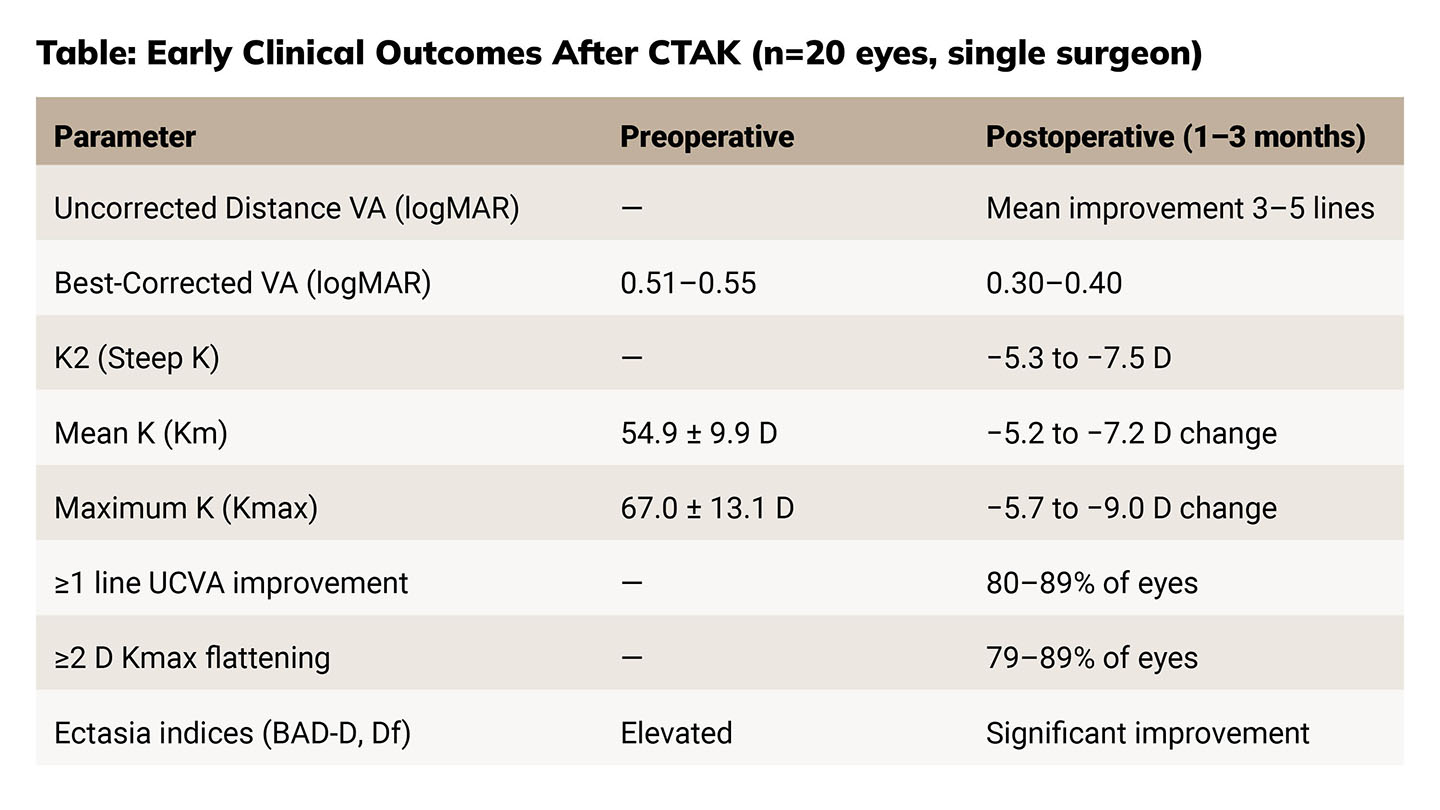
In a prospective trial of CTAK, at 6 months, mean UDVA improved from ~20/327 to ~20/82 and CDVA from ~20/82 to ~20/43, with most eyes gaining ≥2 lines of UDVA and more than half gaining ≥2 lines of CDVA. Mean keratometry flattened by ~8 D, refractive error shifted toward plano, and no eyes lost UDVA, demonstrating meaningful early improvements in both vision and corneal shape.2
Advantages of CTAK include: highly reproducible geometry; greater customization of arc length and thickness; and a simplified intraoperative workflow. However, clinics must coordinate scheduling with an eye bank and face higher tissue-processing costs.
Patient Selection: Who Benefits Most?
Tissue-addition reshaping is best suited for patients between conservative management and transplantation.
Typical candidates include those with:
-
Moderate to advanced KCN with poor spectacle vision
-
Contact lens intolerance
-
Irregular corneas unsuitable for topography-guided ablation
-
Adequate stromal thickness for channel creation
Eyes with dense scarring, extreme thinning, or severe post-hydrops distortion may still be better served by lamellar or penetrating keratoplasty. Patient selection criteria and surgical techniques continue to evolve, making this an active and exciting area of corneal surgery.
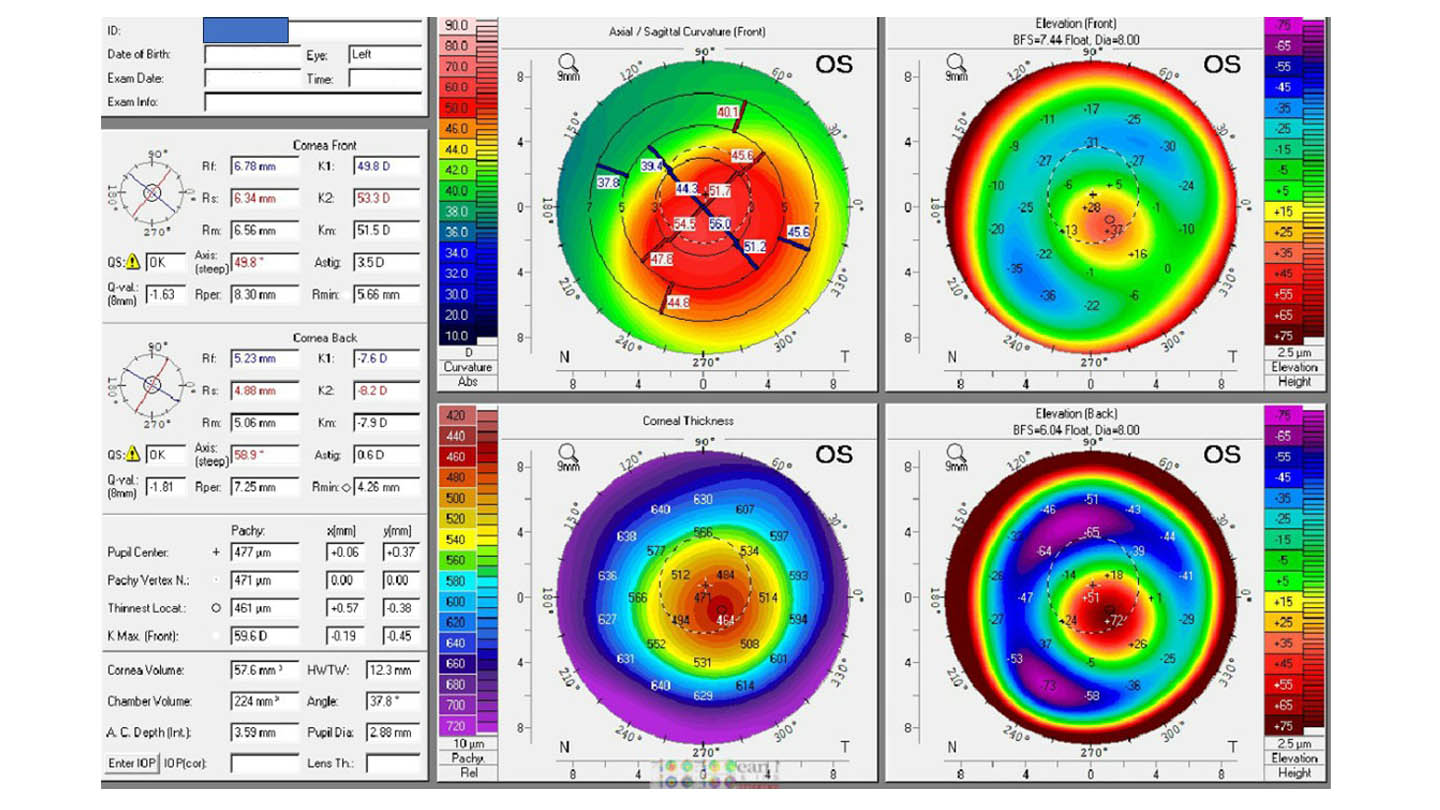
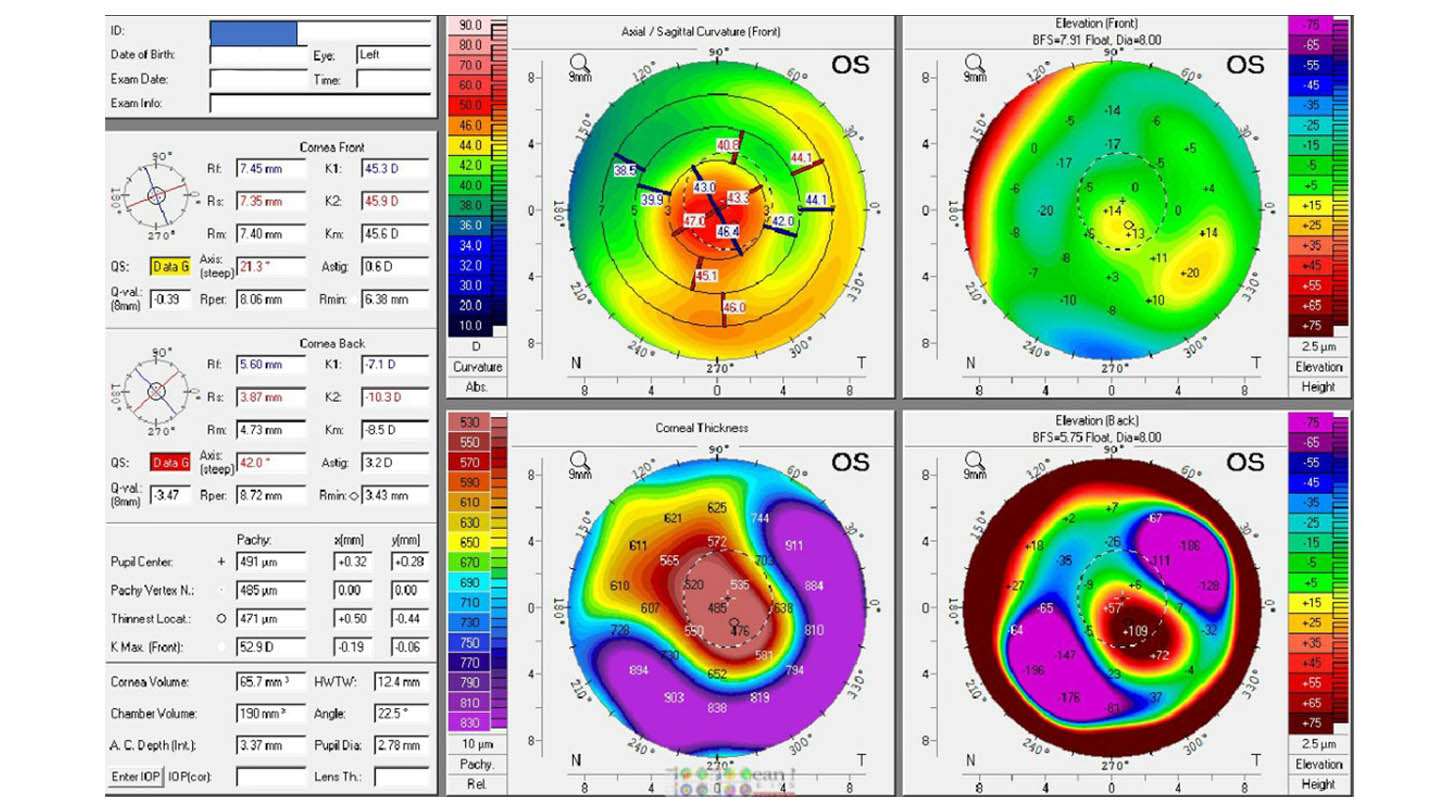
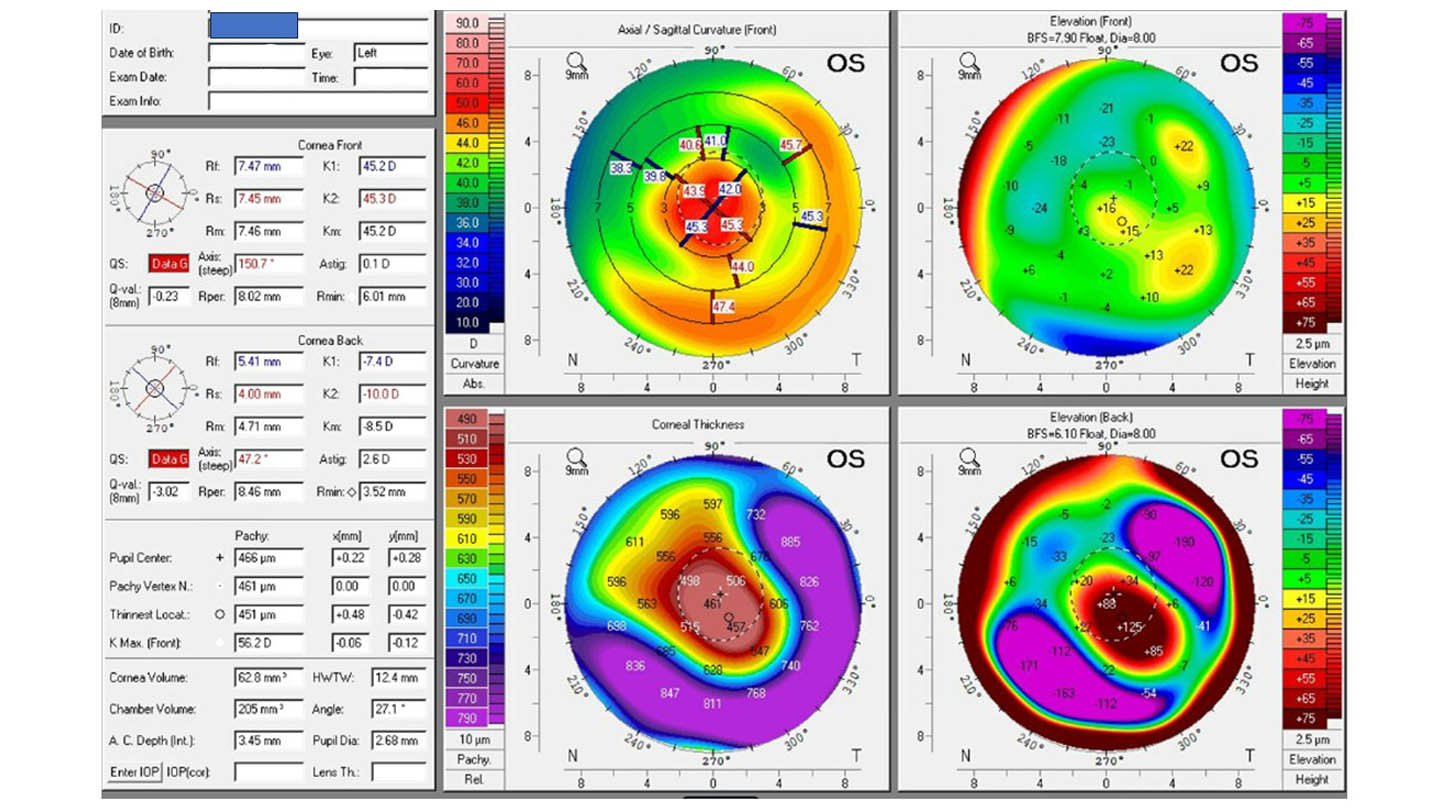
Figures 2–4 illustrate one of my early CTAK case’s preoperative and postoperative outcomes.
Where Corneal Cross-Linking Fits In
CXL is not a reshaping procedure; its role is biomechanical stabilization. In the context of tissue-addition reshaping, CXL helps preserve the newly achieved corneal geometry.
In this context, CXL may be performed either 1) Before reshaping (to halt KCN progression prior to altering corneal geometry) or 2) After reshaping (to stabilize the newly “flattened” cornea)
The sequence depends on age, progression risk, and corneal thickness. Patients should understand that CAIRS/CTAK improve corneal shape, while CXL helps maintain those gains over time.
Tips for Integration of CAIRS and CTAK
Imaging and Planning: High-quality corneal tomography is essential for diagnosis, planning, and postoperative monitoring. CTAK planning typically requires Pentacam imaging. AS-OCT, epithelial mapping, and aberrometry may provide additional useful data.
Surgical Platform: A femtosecond laser capable of creating an intrastromal channel is required. Many refractive platforms support this with software upgrades. Manual dissection remains possible but is less common.
Surgery Logistics: CTAK often involves 2 procedural settings. Channel creation occurs in a laser suite, while tissue implantation, billed as a corneal transplant procedure (CPT 65710), may need to take place in an operating room, depending on payer and facility requirements.
Some practices perform laser and implantation on the same day at different locations, which can be challenging if laser and surgery centers are geographically separated. Others perform implantation 1–2 weeks later, simplifying logistics but requiring careful tissue coordination.
CTAK also requires scheduling coordination with the eye bank to align with tissue delivery windows, and staff familiarity with tissue handling protocols. CAIRS avoids dependence on eye banks but requires surgeons to be comfortable with lamellar tissue preparation, which may limit adoption outside corneal subspecialty practices.
Patient Counseling: Why It Matters
Patients should understand that the goals of these procedures are functional vision improvement, reduced irregularity, and delayed transplantation—not spectacle independence. Additional procedures or contact lenses may still be needed.
Tissue-based corneal reshaping expands treatment options in a way that aligns well with modern anterior segment and refractive practice.
For patients, this means:
-
Fewer years of poor vision or uncomfortable lenses
-
Less invasive options before transplantation
-
Improved quality of life earlier in disease course
Conclusion
Tissue-addition intrastromal reshaping procedures represent a meaningful evolution of the original ICRS concept. By replacing synthetic implants with biologic tissue and enabling customized reshaping without tissue removal, these techniques address many limitations that historically constrained INTACS use.
When combined thoughtfully with CXL for biomechanical stabilization, tissue-based reshaping offers ophthalmologists a powerful new tool to improve vision, enhance contact lens tolerance, and delay transplantation for patients with irregular corneas. As these technologies mature and access expands, they are likely to play an increasingly important role in modern anterior segment practice. OM
References
1. Jacob S, Agarwal A, Awwad ST, Mazzotta C, Parashar P, Jambulingam S. Customized corneal allogenic intrastromal ring segments (CAIRS) for keratoconus with decentered asymmetric cone. Indian J Ophthalmol. 2023;71(12):3723-3729. doi:10.4103/IJO.IJO_1988_23
2. Greenstein SA, Yu AS, Gelles JD, Eshraghi H, Hersh PS. Corneal tissue addition keratoplasty: new intrastromal inlay procedure for keratoconus using femtosecond laser-shaped preserved corneal tissue. J Cataract Refract Surg. 2023;49(7):740-746. doi:10.1097/j.jcrs.0000000000001187