







Throughout history, all medical decision-making has relied upon anecdote, expert opinion and cumbersome, limited clinical trials with delayed or non-existent post hoc analysis and validation. More recently, however, the advent of large, connected datasets and artificial intelligence (AI) has created the exciting potential to optimize and validate medical decision-making. These AI approaches can be applied universally across medicine, with a particularly high expertise currently focused on ophthalmology.
While AI and machine learning have impacted all sectors of our society, medicine is certainly at the forefront because we can so greatly benefit from advances in this field. We have made astounding progress in the decade since we realized the power of AI, which has become indispensable to image analysis, predictive algorithms and guidance across all fields of medicine.
Today, AI is used in ophthalmology primarily for screening of diseases such as glaucoma, diabetic retinopathy, macular degeneration, cataract and keratoconus.
My colleagues and I founded Advanced Euclidean Solutions (AES) about 10 years ago, when we realized that the power of AI would ultimately surpass human ability to write an algorithm or formula for any medical mathematical problem. Our vision went from simply predicting an outcome to guiding the physician to better outcomes. In addition, we believed (and still do) that adjustments of practice patterns are best made with deep learning and incremental changes to a field of medicine.
Recently, AES was awarded a U.S. patent for the novel methodology to improve IOL calculations using AI that includes an in-the-cloud device to seamlessly refine all formulas or approaches to these refractive calculations. Here’s how we applied our beliefs to bring the power of AI to eye care.
Beyond the A-constant
Once we understood that AI could continually improve in perpetuity, we began applying this concept to other areas of ophthalmology, including corneal refractive surgery and macular degeneration. The key to progress is continued learning from large data sets gleaned from surgeons across the globe.
While this may seem obvious now, it wasn’t when AES began our work a decade ago. We started in 2015 by publishing in JAMA Ophthalmology an original paper on IOL calculations1 that demonstrated how we could think of formulas in multiple dimensions. Our work rapidly advanced as we realized we could adjust any formula, now or in the future—whether it be vergence, thick or thin lens-based, paraxial ray-based or even AI-generated.
For IOL calculations, surgeons for the past 40 years have relied on adjusting A-constants to improve their surgical results. This has been achieved by relying on individual postoperative refractive results or a database of many surgeons (such as the online ULIB database). In fact, if a surgeon didn’t adjust their A-constant and just used what was labeled on the box, it would have been considered sub-standard care. It is now well known that adjusting an A-constant equally for all types of eyes is inadequate, and surgeons and industry have recognized this.
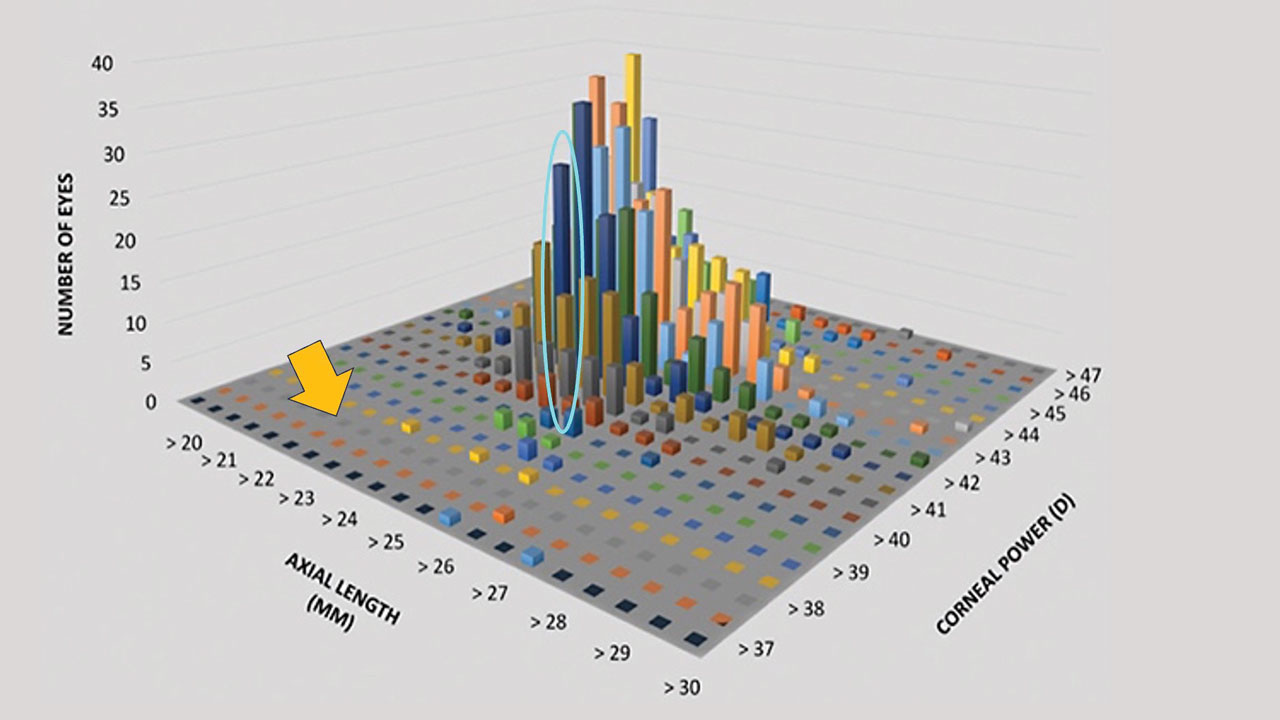
Figure 1 demonstrates why this no longer makes sense. It shows that AI
algorithms of just three known variables can produce 1,000 individual points on a matrix. All of these variables influence the success of the formula and are intimately related. No human being alone could adjust a formula for a specific eye.
Evolving Algorithms and Formulas
While the concept was simple and elegant, the algorithms we initially used were in their early stages of development. Since then, the algorithms to achieve our “adjustments” have become more sophisticated and have continued evolving. In addition, coding of these programs has become easier and more efficient with large language models (LLMs) to help with the process.
Our patent involves AI-based optimization of any formula (including our own) for calculating IOL power in cataract surgery. In addition to working on any formula, the IP is secured for working on as few as two input variables (i.e., axial length and corneal power) or an infinite number of variables that exist now or will ever exist. One facet of our methodology is that no matter what formula one starts with, as more outcomes and variables are introduced over time, all formulas will evolve into one perfect formula, which we call the Singularity™.
The allowed patent also includes a cloud-based device that accumulates and stores data and uses our methodology to improve itself. Although these allowed claims are separate, they are both important to securing the most likely and efficient way for the data and the process to evolve.
We’re Not Done Yet
Although this was our first patent, we have others in the pipeline that will help our field and our patients over time.
Our intellectual property in corneal refractive surgery is similar to the IOL calculation patent in that it uses outcomes to adjust future treatment plans with deep learning.
Our retina projects are a bit different. They help to predict the outcome of various treatments and guide future interventions as new modalities come into existence in a continually self-
optimizing algorithm. This is akin to navigational applications like Waze and Google Maps, which are constantly calculating the best route to take to a particular destination. Another analogy is playing chess with a chess engine by your side.
We are at a point in medicine where physicians can use AI and deep learning as part of what is called “distributed cognition”— the theory describing how information processing is spread across people, their environments and their tools. We believe more than ever that this is a pathway to better outcomes in all fields of medicine, especially ophthalmology. OM
Reference
1. Ladas JG, Siddiqui AA, Devgan U, Jun AS. A 3-D “Super Surface” Combining Modern Intraocular Lens Formulas to Generate a “Super Formula” and Maximize Accuracy. JAMA Ophthalmol. 2015;133(12):1431–1436 doi:10.1001/jamaophthalmol.2015.3832
