







THE TAKE-AWAYS
Advice for implementing standalone MIGS:
- Glaucoma surgeons should build confidence in offering MIGS by selecting appropriate patients based on their disease severity and response to prior treatments.
- Integrating MIGS into the treatment algorithm allows for a more comprehensive and personalized approach to glaucoma management.
- Ongoing evaluation of patient response and continuous optimization of outcomes are essential components of successful MIGS implementation.
- Patient satisfaction is key to the success of standalone MIGS procedures and practice growth.
- Glaucoma surgeons should leverage positive patient experiences by encouraging them to share their success stories, thereby generating word-of-mouth referrals.
- Tracking outcomes and collecting patient testimonials provide valuable evidence of the procedure’s efficacy and patient satisfaction.
Recent advancements in glaucoma management have introduced micro-invasive glaucoma surgery (MIGS) as a safe and valuable standalone procedure.1 In this article, we will delve into the case for performing MIGS on its own rather than waiting until the patient requires cataract extraction (for more on performing MIGS with cataract surgery, click here). We will also examine how to effectively communicate the safety and value of the procedure to patients, equipping practices for standalone MIGS procedures as well as preparing staff, as well as take a look at the available MIGS technologies.
MIGS VS MORE MEDICATION
Why do standalone MIGS rather than simply add another drop? In a number of scenarios, standalone procedures are very much in the glaucoma patient’s interest. For example, when the patient:
- Is tolerating as many medications as they can and already had a laser procedure, but they need additional pressure lowering due to signs of progression or being far from their target pressure.
- Is experiencing issues with ocular surface disease and are using other prescription drops to treat dry eye. Eye-care providers need to lower their IOP, but their corneal surface discomfort or vision problems have one wanting to avoid adding another drop. MIGS provides the opportunity to do something that would not only help lower their pressure, but may also reduce their medication burden, which could help the ocular surface and enhance vision.
- Has difficulty remembering to keep up with their drop regimen, such that one day their pressure is under control but another day it’s not.
- Is having trouble getting their medications from the pharmacy for reasons such as cost or it is unavailable.
- Finds it difficult to instill the drops physically.
So, we are no longer necessarily looking for maximum tolerative therapy to be comprised of all the various classes of medicines. Adding another medication is not better if patients already have problems with the medications they are currently on. Open communication with patients is crucial to identify if standalone therapy would be more beneficial for their individual needs.
MIGS MESSAGING FOR PATIENTS
Effective communication is paramount in ensuring patients understand the value of MIGS. Simplifying complex medical terminology and utilizing visual aids can significantly enhance their comprehension. Clear and concise explanations should address patient concerns and misconceptions, allowing them to make informed decisions about their treatment.
When the patient comes in and I find their glaucoma is progressing, I explain the treatment options. We can add another drop, but I tell them why that might not be ideal for them. For example, they may be on a lot of drops already, their ocular surface may be compromised or I may not be confident that a single drop will get them to their target IOP.
Then, I address the possibility of laser treatments. But perhaps they’ve already had a laser treatment and it didn’t work well long enough, or I might not be certain it’s going to reduce the number of drops they’re on.
Next comes the surgical discussion. I explain that there are various surgical options available, and after assessing their eye anatomy, I believe they could be an ideal candidate for MIGS. I inform the patient that this procedure aims to gently open their natural drainage system, creating a stable conduit for improved drainage and lower IOP, which can lead to longer-lasting results in maintaining an open drainage pathway.
I explain that MIGS can be performed as a standalone procedure, which is generally well-tolerated, involves no sutures and offers a relatively quick healing time. For patients who have undergone cataract surgery, I can emphasize that the MIGS procedure is comparable to a routine cataract surgery in terms of simplicity and recovery.
As you discuss the possibility of MIGS with the patient, it is crucial to highlight its safety profile, including its low complication rates and favorable outcomes compared to traditional glaucoma surgeries.1,2 Patients should be made aware that MIGS is minimally invasive, resulting in shorter recovery times and reduced postoperative discomfort.
A LOOK AT AVAILABLE TECHNOLOGY
The MIGS devices
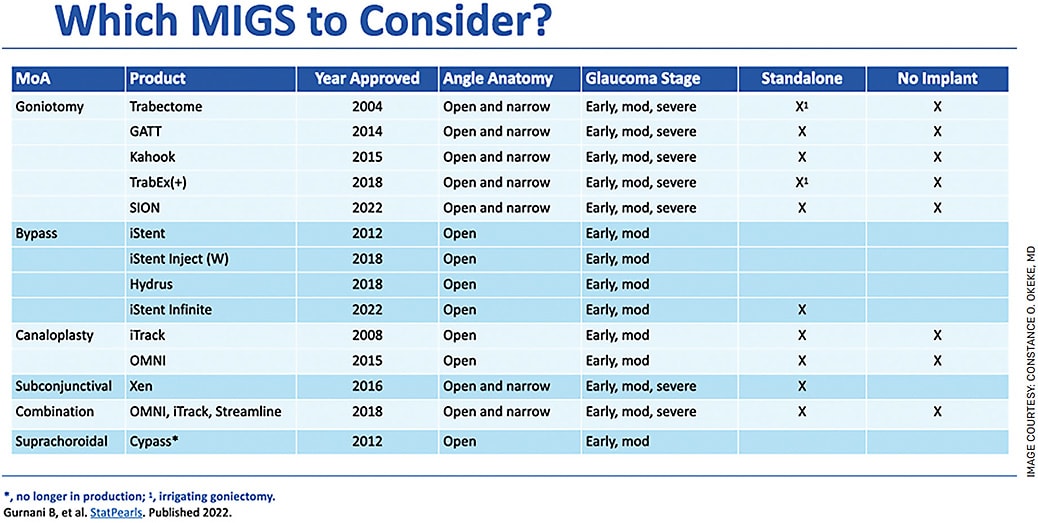
MIGS encompasses a range of devices, each with its own unique mechanism of action. Goniotomy procedures that unroof the trabecular meshwork include devices such as Trabectome (MicroSurgical Technology), Kahook (New World Medical), TrabEx (+) (MicroSurgical Technology) and SION (Sight Sciences). These can be utilized for up to 180° of treatment and GATT, or gonioscopy-assisted transluminal trabeculotomy, which can be used for up to 360°. Viscodilation or ab interno canaloplasty with devices such as iTrack Advance (Nova Eye Medical) can provide another approach to enhancing outflow by dilation and adhesion removal of the Schlemm’s canal, outflow collector channels and trabecular meshwork.
Combined mechanisms for enhanced outflow can be further achieved with devices such as the OMNI Surgical System (Sight Sciences) and STREAMLINE Surgical System (New World Medical) that open trabecular meshwork and deliver viscoelastic to the outflow system. Trabecular meshwork bypass devices, such as the iStent infinite (Glaukos), consisting of three stents and now FDA approved for standalone usage, create a direct pathway through the trabecular meshwork for aqueous humor outflow, thus reducing IOP.1
Subconjunctival devices and implants, including the XEN Gel Stent (Allergan), divert aqueous humor to a subconjunctival reservoir, providing an alternative pathway for drainage. Mitomycin is required for the success of the bleb creation.
When considering the available MIGS technologies, it is crucial to evaluate factors such as efficacy, safety and long-term outcomes. Each device has clinical evidence supporting its use, and glaucoma surgeons should consider the patient’s unique characteristics and preferences when selecting the most appropriate device.3,4
Angle vs subconjunctival vs combination
When I consider the different offerings of angle-based vs subconjunctival-based vs combination therapy, I evaluate the patient based on their type and stage of glaucoma, how many drops they are currently on, what their target pressure is, how far off they are from that target, what their angle anatomy looks like — if it’s pristine or if there’s pathology present, such as synechiae or increased pigment — as well as their conjunctiva and any previous surgeries (Figure).
MY MIGS ALGORITHM
Integrating MIGS into the treatment algorithm allows for a more comprehensive and personalized approach to glaucoma management. I typically offer selective laser trabeculoplasty (SLT) or drops as initial therapy. I lean toward SLT, because I feel it’s more impactful the earlier it’s used. Then, I would follow with drops — usually once daily and a prostaglandin analog.
If that does not get the patient to target, I consider Durysta (sustained-release intracameral bimatoprost, Allergan). Durysta is an option when patients are interested in fewer drops, such as after SLT and would like to avoid a daily drop, or if the patient is already on multiple drops and we want to lighten the load in terms of cost or ocular surface dryness as well as the desire to reduce the side-effect profile.
Standalone MIGS come into play when patients have already had SLT and are either not at the level I feel it’s going to be repeatable or that the efficacy won’t get them to target. The patient is already on two or more drops. Standalone MIGS is typically for patients who are mild to moderate.
There’s also the opportunity to use cyclophotocoagulation. I add an MP3 laser there and usually do that in patients who are hesitant to have a surgical procedure but know they need to do something, and maybe they’ve already had SLT.
Some procedures can be done for just open angle, while others can be done for narrow angle or a combination. When it comes to standalone procedures, I typically used non-stent procedures until recently. We now have the iStent infinite, which I use in patients who have open angles and more moderate to severe disease.
I usually reserve subconjunctival-based surgeries for glaucoma patients who have already had some type of MIGS angle surgery and are now on multiple medications. These subconjunctival patients are often on at least three classes of medications. They are off their target, in fact, not uncommonly far from the target — 10, 20 points away. They have good conjunctiva that’s very freely mobile in the superior nasal area; their angle is amenable to being accessed in an internal or also could be an external approach. For instance, if a patient has a previous corneal graft and I’m hesitant to do anything internal, I can do an external insertion of a subconjunctival stent, avoid the cornea and still get an excellent result.
So, my subconjunctival-based stents are usually reserved for patients whose pressures need a significant reduction to achieve target, are on quite a number of medications and have moderate to advanced glaucoma.
In terms of combination therapy vs angle based, I lean towards doing more combination therapies than angle-based procedures, because I find that the goniotomy plus visco-dilation approaches seem beneficial not just for high-pressure reduction, but I see less hyphema with this combination, less long-term inflammation and good efficacy.
PREPARE YOUR PRACTICE/ASC FOR STANDALONE MIGS
First, research
To offer standalone MIGS procedures confidently, glaucoma surgeons need appropriate training and expertise. Recognizing that there is a learning curve associated with MIGS, it is essential to seek out training opportunities with colleagues and industry experts.
There are a number of resources doctors can go to that will help give them the confidence to adopt new procedures. Physician YouTube channels are a great example. I created the iGlaucoma YouTube channel, where I post videos that help educate doctors on glaucoma surgical techniques — not just the steps but also common challenges surgeons might face. I have a series of videos called “MIGS Success Surgical Secrets” that highlights a number of different MIGS procedures and the challenges surgeons may face performing them and how to overcome them.
Staff outreach
Conversations about incorporating a new technology should start with your management team. ASC and clinic management evaluate the product to find out if it’s going to be utilized and well reimbursed. After learning the billing process, the practice might perform a trial with a certain number of patients. Medicare patients are usually well covered for most procedures, so they might make good candidates.
Once that trial is decided, it’s time to talk to staff. They need to know there’s a new technique that’s being adopted and have a general understanding of how the procedure works and why you would do it. Show them a video or marketing materials, and be sure to share your excitement about the device. Staff should also be coached on how to answer questions from patients.
Include scribes and surgical schedulers in staff education efforts as well, because certain things must be done. New consent forms must be created as well as brochures for the patients, and a specific date for the trial of the procedure must be established. Before settling on a trial date, confirm with the rep for that procedure to make sure they are available and coordinate any previous wet lab that might need to be done prior.
You must also ensure that the ASC staff are appropriately trained, as a new technology sometimes requires certain techniques to be performed. Moreover, practices and ASCs must ensure they have the necessary infrastructure and equipment to accommodate MIGS procedures. This may involve making modifications to the surgical environment, acquiring specialized instruments and optimizing the workflow to enhance efficiency. Implementing protocols for patient selection and preoperative evaluation will further contribute to successful outcomes.
Now get the word out
If the result of that trial leads you to decide to continue offering MIGS, you need to reach out to your referral network. That may include explaining to other doctors that you have started using this new procedure, giving them an explanation and describing who are good candidates. This could be a dinner lecture where you bring in referral doctors and you talk about the procedure or a sponsored event or tie in with some kind of CME event for the practice.
It helps to educate the community as well. This can involve something as simple as including announcements of new MIGS procedures in your on-hold message system so that patients hear about it when they call. Use social media to publicize MIGS too, especially if you are the first in your community to offer it. Leverage positive patient experiences by encouraging them to share their success stories on the practice’s social media as well, thereby generating word-of-mouth referrals.
CONCLUSION
Glaucoma management is becoming increasingly interventional. We know that there are issues related to medication compliance. Medication management is not going away, but we are trying to utilize fewer medications because we know the burden they place on patients — the cumbersome drop regimens, the corneal surface issues they cause and the question of cost.
As advancements in MIGS technology continues, standalone MIGS procedures hold promising prospects for the future of glaucoma management. Ongoing research and innovation will likely result in the development of new devices and techniques, further expanding the treatment options available to glaucoma surgeons and relieving our patients of the problems associated with drug therapies. By incorporating these advancements into their practices, ophthalmologists can provide optimal care and enhance patient outcomes. OM
This article is being published in collaboration with the AGE Initiative, a global movement to creatively prevent worldwide glaucoma blindness. For more information go to www.DrConstanceOkeke.com/AGE-Initiative .
REFERENCES
- Samuelson TW. Prospective, randomized, controlled, pivotal clinical trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2015;122:1122-1131.
- Gedde SJ, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153:789-803.
- Saheb H, Ahmed IIK. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96-104.
- Voskanyan L, García-Feijoó J, Belda JI, et al. Prospective, unmasked evaluation of the iStent inject system for open-angle glaucoma: synergy trial. Adv Ther. 2014;31:189-201.
- Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124:1579-1588.
