







The IC-8 Apthera IOL is the first and only non-toric EDOF lens approved to treat cataracts and up to 1.5 D of astigmatism.
Monovision remains a common method for correcting presbyopia with laser vision or implant-correcting surgery. It’s well tolerated among patients, but the modality is not exactly intended for everyone. This is particularly true for a dual diagnosis of cataracts and astigmatism.
Physicians might find themselves utilizing monovision even more frequently with the introduction of a new IOL, however. Approved by the FDA in late July, the IC-8 Apthera IOL (AcuFocus Inc.) could impact the industry in a way that’s unique from previous IOLs.
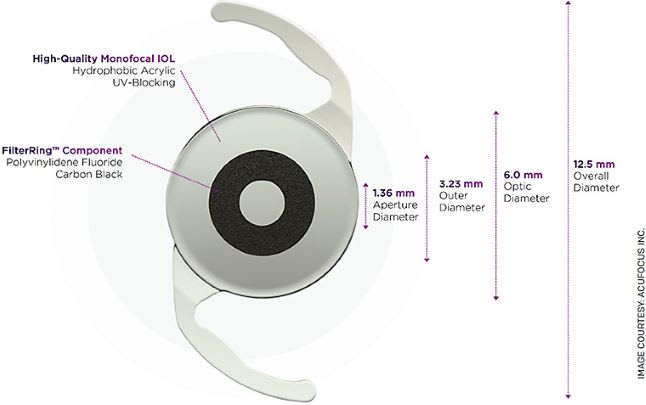
The first and only non-toric extended depth of focus (EDOF) lens approved for the treatment of cataracts in patients who also exhibit up to 1.5 D of corneal astigmatism, the Apthera IOL also has some physicians envisioning an “advanced” or “extended” form of monovision. A small aperture lens that filters out peripheral defocused, or aberrated, light while allowing only focused light to reach the retina, the IOL has shown an ability to improve uncorrected intermediate and near vision as well as equivalent distance vision and contrast sensitivity in a recent US Investigational Device Exemption (IDE) Study. “We’ve been waiting for a small aperture IOL to receive FDA approval,” says Vance Thompson, MD, director of refractive surgery at Vance Thompson Vision in Sioux Falls, S.D., and a trial investigator. “What’s so beautiful about this lens is that it improves both cataract blur and cornea blur.”
NEW CHARACTERISTICS
In addition to some of the other firsts mentioned above, the Apthera IOL is also the first lens indicated for implantation alongside a monofocal or monofocal toric IOL in the fellow eye.
The FDA approval is based on the IDE, which evaluated the safety and effectiveness of the IOL implanted in one eye among patients with a monofocal or monofocal toric IOL implanted in the other eye. A total of 453 subjects were followed for 12 months and compared to a control group that received a monofocal or monofocal toric IOL in both eyes. Eyes treated with Apthera maintained 2.0 D of EDOF and demonstrated 0.9 D of additional range-of-vision benefit over the monofocal IOL at a logarithm of the minimum angle of resolution (logMAR) threshold of 0.2, exceeding the 0.5-D criterion set by the American National Standards Institute for EDOF lenses. Apthera IOL subjects also achieved comparable binocular contrast sensitivity to control subjects in both photopic and mesopic conditions, a first for an EDOF lens, according to AcuFocus.
“The availability of this novel small aperture design will give surgeons and patients a completely different mechanism of action to work with to improve vision after cataract surgery,” says Yari Mitchell, chief business development officer.
UNMET NEEDS FINALLY MET
According to Dr. Thompson, the concept of a monofocal or a monofocal toric in the distance eye and the reading lens in the other eye is especially intuitive.
“It’s an unmet need — many doctors who have not been comfortable with multifocal implants who still utilize monovision as their primary way of taking a cataract patient and postoperatively giving them a functional near image have to blur distance a lot to do that,” he says. “And for the many surgeons who prefer monovision but have patients with a blurry distance eye who can’t tolerate it, they either have to exchange the implant or do laser vision correction over the cornea. But with this lens, the reading eye actually has distance vision that is quite good and balances well with the good distance produced in the other eye. This will help doctors make monovision more precise. Our study involved patients with up to 1.5 D of corneal astigmatism, and these patients also achieved quality distance, intermediate and near vision because of the way small aperture optics focus light.”
Another unmet need the lens addresses, says Dr. Thompson, is among patients seeking full range of vision and spectacle independence — there is less of a chance of needing a laser refractive enhancement with this lens. “Small aperture optics provide for quality visual function at distance, intermediate, and near — even in the presence of low levels of refractive error after cataract surgery,” he says.
The lens’ FilterRing component, an embedded opaque annulus, creates a reduced aperture in the eye that filters away the defocused light, which is often responsible for degrading image quality and vision range. As a result, patients can see more clearly from far through intermediate to near without visual field loss, explains Ms. Mitchell.
BOTH ART AND SCIENCE
The impact of the lens in clinic could allow physicians to reevaluate their approach to monovision, says William F. Wiley, MD, with Cleveland (OH) Eye Clinic. “As we see multiple ways of correcting presbyopia with the use of accommodating lenses, bifocal lenses, trifocal lenses, EDOF, diffractive EDOF, zonal EDOF and now aperture EDOF — these different optical principles will be applied to patients for different options,” he says. “You can get caught up in talking about the technology to patients, but what is more practical is teasing out what the patient’s goals are. That’s using the ‘art’ of satisfying the patient and managing expectations.”
As an example, Dr. Wiley offers a patient who’s experienced fluctuating vision, cataracts, glare and halo after radial keratotomy.
“The Apthera IOL might solve these multiple problems,” he says. “It can take care of the cataract, extend the focus for near vision, allow for a softer landing if vision is fluctuating, is more tolerant to refractive error and can filter out irregular astigmatism that the incisions were inducing.”
Dr. Wiley also believes there’s potential to improve the ease of pre- and intra-operative diagnostics on surgical guidance.
“With a premium lens, we’re focused on management of astigmatism, which is dependent on effective use of preoperative diagnostics and surgical intraoperative guidance,” he says. “For most lenses to function and perform properly, one must have the astigmatism tuned tightly. This lens is forgiving and tends to tolerate low or medium amounts of astigmatism. There’s no toric correction alignment required, so it may allow for a more efficient throughput. There could also be some nuanced preoperative testing to simulate what the aperture might look like for different patients. It will be interesting to see how this all comes into play.” OM