







One could be forgiven for thinking that IOP is part of the definition of glaucoma, given how often we talk about IOP when managing patients with glaucoma. Indeed, IOP is the only known modifiable risk factor for the prevention or treatment of glaucoma, and all our therapies for glaucoma — such as topical and oral medications, laser and surgical procedures — are designed to lower IOP.
This begs the questions: How are we measuring IOP, and how much do we really know about each patient’s IOP?
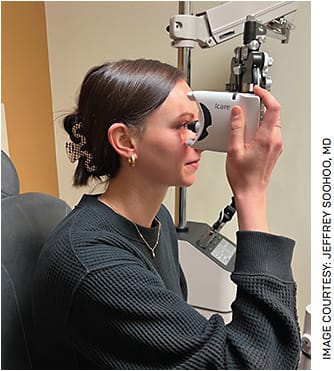
The iCare HOME (ICare USA) self-tonometer promises to exponentially expand our knowledge. Introduced in the United States in 2017, the device is a rebound tonometer that measures IOP via the deceleration and contact time of a lightweight probe that makes momentary contact with the cornea and does not require topical anesthesia for use.
THE LIMITATIONS WE’VE BEEN PRACTICING UNDER
The gold standard for measuring IOP is the Goldmann Applanation Tonometry (GAT) performed at the slit lamp during an office visit. For most patients, however, this means that IOP is measured for a few seconds two to four times a year — during office hours, of course. What, then, is happening during the time between visits and outside office hours? IOP is dynamic, and in-office IOP readings are unlikely to truly capture a patient’s range of IOP, pattern of fluctuation or peak IOP.
One study found that 69% of patients have a peak IOP reading outside of office hours!1 Data such as these suggest that our current practice patterns don’t give us the whole story about IOP.
Until recently, we did not have many viable options for gathering more IOP data. One could perform serial tonometry in the office to have more data points throughout the day, although these readings would still reflect only a patient’s IOP during office hours. For readings outside of office hours, patients can be referred to a sleep laboratory for overnight testing, but this is a labor-intensive undertaking and is not a scalable practice. Other options for remote and/or continuous IOP monitoring, such as a contact lens, have not yet proven feasible on a large scale.
With iCare HOME, we have self-tonometry. While some might be concerned about the accuracy of the technology, studies have shown that the iCare HOME leads to IOP measurements that are similar to those obtained by GAT, with the majority of patients agreeing that the device is easy to use and comfortable.2,3
PATIENT SELECTION
While it would be advantageous to have additional data points on all patients, this is not practical in most practices. In my own, I have specific patients for whom I prefer to obtain a week of home IOP measurements, if possible.
First are treatment-naive patients who are newly diagnosed with glaucoma or ocular hypertension. This group benefits greatly from home tonometry as it provides a more comprehensive understanding of their baseline IOP, which allows for a better assessment of treatment response and the setting of a target IOP.
Next, I try to obtain home tonometry before and after treatment escalation, such as the addition of another topical medication or surgical intervention. These additional data points are helpful to assess the response to the treatment escalation and often provide additional impetus for more aggressive treatment if IOP variations or peaks are significantly different from those noted in the clinic.
Finally, I find home tonometry most valuable in patients with glaucoma that is progressing despite clinic IOPs that are consistently at or below the patient’s target IOP. While IOP-independent mechanisms of glaucoma progression are not well understood, I often find that these patients have significantly higher IOPs on home tonometry, particularly at times outside of normal office hours.
In these cases of progressing glaucoma, knowing the true range of IOP gives both the provider and patient peace of mind that there is a potential explanation for the glaucomatous progression and supports more aggressive treatment.
NEW DATA
A recent study from my colleagues at the University of Colorado helps to shed light on the ability of iCare HOME to detect a treatment response in patients with glaucoma or ocular hypertension.4 This study was a prospective clinical trial that divided 43 patients into four groups:
- Stable medical management of IOP with no planned change in therapy (control)
- Planning for selective laser trabeculoplasty
- Starting first topical IOP-lowering medication
- Adding a second topical IOP-lowering medication to existing monotherapy
Each group had a baseline visit with IOP measurement by GAT and training with the iCare HOME device. Participants then took four IOP measurements at home each day for 1 week, after which the planned change in therapy was initiated (with the exception of Group 1). Four to 6 weeks later, patients repeated the 1 week of at-home IOP measurements. A final clinic visit then measured IOP by GAT and downloaded iCare HOME data.
As expected, the control group had no change in IOP. Treatment-escalated patients were labeled as responding to treatment if their pre- and post-intervention by GAT was significantly lower. Those without a significantly lower IOP by GAT in the office were labeled as non-responders. When this second group’s iCare HOME data was analyzed, however, three of the four daily time points were found to be significantly lower than pre-intervention IOPs.
The study concluded that measuring IOP by in-office GAT may underestimate a patient’s true response to treatment.
ISSUES TO RESOLVE
Practices may struggle with the costs of the iCare HOME device and the disposable probes as well as the time needed to train patients (Figure). At my practice, we allot 15 to 30 minutes for instructing patients in correct usage. We find the most common difficulties patients have are maintaining proper position and blinking.
Fortunately, CPT codes are now available for remote patient monitoring (99453, 99454, 99457) that allow for reimbursement for these services. Note, however, that these codes are not specific to IOP measurement and require that certain conditions be met for reimbursement to occur. For instance, CPT 99457 requires at least 20 minutes of interactive virtual care during the month in which the code is billed. CPT 99454 requires at least 16 days of device readings during the 30-day period for which the code is billed.
Home tonometry using iCare HOME is not a perfect solution; the device is dependent on patients being able to use the device appropriately, and some patients, for a variety of reasons, are unable to consistently obtain accurate measurements. Due to the cost of both the device and the disposable probes, a practice planning to implement home tonometry must explore options to mitigate these costs and create the appropriate workflows for reimbursement. Our practice either uses the CPT codes mentioned above or gathers these data as part of established research protocols.
iCare HOME also cannot provide IOP data when patients are asleep or performing particular activities such as strenuous exercise. Because the data collected are periodic data points, the physician still does not have access to continuous data.
GET A BETTER PICTURE
Having the option to understand a patient’s true range of IOP readings across multiple days and outside of office hours is an invaluable tool in the management of glaucoma. Patients uniformly appreciate the opportunity to more actively participate in gathering data that informs their care plan. Home tonometry also has the potential to reduce office visits for patients, especially those who must travel significant distances to seek ophthalmic care.
Ultimately, the advantages of home tonometry outweigh any disadvantages; the time has come to expand our understanding of a patient’s IOP to times outside of office hours on a more consistent basis. OM
REFERENCES
- Barkana Y, Anis S, Liebmann J, et al. Clinical utility of intraocular pressure monitoring outside of normal office hours in patients with glaucoma. Arch Ophthalmol. 2006 Jun;124:793-797.
- Dabasia PL, Lawrenson JG, Murdoch IE. Evaluation of a new rebound tonometer for self-measurement of intraocular pressure. Br J Ophthalmol. 2016;100:1139-1143.
- Pronin S, Brown L, Megaw R, Tatham AJ. Measurement of intraocular pressure by patients with glaucoma. JAMA Ophthalmol. 2017;135:1030-1036.
- Scott AT, Kanaster K, Kaizer AM, et al. The utility of iCare HOME Tonometry for detection of therapy-related intraocular pressure changes in glaucoma and ocular hypertension. Ophthalmol Glaucoma. 2022;5:83-93.
