







Pediatric ophthalmology and strabismus have a diverse, rich and complex history in the story of medicine. Although officially recognized by educational institutions, medical societies, specialty organizations, medical literature and governmental agencies, its providers, patients, practice needs and important discoveries are often eclipsed by the concerns of adult ophthalmology. Nowhere is this more evident than the consistent lack of pediatric ophthalmology and strabismus as a choice of career by ophthalmology residents.
Despite this, pediatric ophthalmology and strabismus is one of the most rewarding areas of medical and surgical practice. We are challenged by, and expected to care for, patients with diseases in all areas of the developing visual system and are required to have and maintain broad diagnostic and surgical skills.
It is my pleasure to try and recap the last 25 years of noteworthy events, discoveries and contributions made by hundreds of dedicated men and women who have chosen to practice or investigate the discipline of pediatric ophthalmology and strabismus (with apologies in advance for missing any key contributors or events during the last quarter century).
SOCIETIES
The success of the American Association for Pediatric Ophthalmology and Strabismus (www.aapos.org ) during the last 25 years consists of a commitment to continuing education, subspecialty training, research and community service. This is evidenced by an increasing, although practice restricted, membership from 78 in 1974 to 2,014 in 2021, a bimonthly journal, an independent board of directors, officers and more than 40 committees with primary pediatric vision care representatives to state and local government, the American Medical Association, the American Academy of Pediatrics, the AAO and national and international strabismological and orthoptic societies.1
Under the leadership of Drs. Ken Nischal and David Granet, The World Society of Pediatric Ophthalmology and Strabismus (WSPOS) was established in 2008 to fill the need for an international pediatric ophthalmology and strabismus society recognizing that most of the international eye care in children is performed by adult professionals who also see children. WSPOS (www.wspos.org ) has more than 3,800 worldwide members from 60+ countries with active executive, scientific, ethical and connectivity bureaus. As part of its international mission, WSPOS is a charity without membership costs. Its seminars are part of many international ophthalmological society meetings such as ESCRS, ASCRS, AAO, WOC and SOE. WSPOS also executes a biyearly international congress attended by more than 1,000 delegates representing over 50 countries as well as monthly webinars and instructional courses.
These societies function as hubs for national (AAPOS) and international (WSPOS) distribution of relevant new policies, procedures, discoveries, skill transfers, continuing education, patient and family resources and “connectedness” of professionals dedicated to the visual systems of infants and children.
As an adjunct to society connectedness, and for over 25 years, Dr. Granet initiated and has maintained the largest pediatric ophthalmology online “listserve” with more than 2,500 international contributors.
MULTICENTER CLINICAL TRIALS
The most impactful multicenter clinical trials in pediatric ophthalmology and strabismus have been sponsored by The National Eye Institute (NEI)/National Institutes of Health (NIH).
One example of these collaborative efforts is the Pediatric Eye Disease Investigator Group (PEDIG), a multicenter network of more than 200 pediatric ophthalmologists and optometrists across North America, including private practice and academic institutions. Started in 1997 by Dr. Roy Beck in partnership with Drs. Jonathan Holmes and Michael X. Repka and run by The JAEB Center for Health Research in Tampa, Fla.,2 PEDIG has performed more than 45 studies resulting in more than 120 publications changing practice patterns in the treatment of amblyopia and strabismus. Topics include equal effectiveness of 2 hours of suggested patching compared to 6 hours for moderate and 6 hours compared to full time for severe amblyopia; equal effectiveness of daily and week-end atropine to patching for moderate amblyopia; the use of spectacles alone in the treatment of amblyopia; and effectiveness of amblyopia treatment in older children.
Additional contributions by the PEDIG group in the understanding and management of other disorders include infantile esotropia, intermittent exotropia, childhood cataracts and glaucoma, nasolacrimal duct obstruction, anti-VEGF therapy for retinopathy of prematurity (ROP) and optic neuritis in childhood.3-6
AMBLYOPIA
Many amblyopia studies completed during the last decade involve dichoptic stimulation, a binocular approach where images are presented separately to each eye.7 Luminopia One is the first FDA-approved digital dichoptic amblyopia therapy in children. Patients choose TV shows and movies using proprietary algorithms that modify the selected videos in real-time within a virtual reality headset to promote weaker eye usage and encourage patients’ brains to combine input from both eyes.
RETINOPATHY OF PREMATURITY
Modern knowledge regarding the epidemiology, screening, pathophysiology, prognostic factors, diagnosis, classification, and effectiveness of ROP treatment modalities is primarily the result of collaborative efforts from many study groups.8 These include International Committee for the Classification of Retinopathy of Prematurity, Cryotherapy for Retinopathy of Prematurity, Light reduction in retinopathy of prematurity, Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity, The United Kingdom, Australia and New Zealand Collaborative Groups, Early Treatment of Retinopathy of Prematurity, Bevacizumab Eliminates the Angiogenic Threat of Retinopathy of Prematurity, Post-Natal Growth and Retinopathy of Prematurity Studies, Telemedicine Approaches to Evaluating Acute-phase Retinopathy of Prematurity and Ranibizumab Versus Laser Therapy For The Treatment of Very Low Birthweight Infants With Retinopathy of Prematurity.
Globally, at least 50,000 children are blind because of ROP. In the United States, even with many advances in ROP treatment, approximately 600 premature infants become legally blind each year.
During the last 5-10 years, intravitreal anti-VEGF therapies (Figure 1) have been successfully used to treat ROP.9-11 None of these drugs are FDA approved. An updated classification system and accelerated use of telemedicine are becoming the standard of care in the diagnosis and study of ROP.12,13

Figure 1. Neonatal intraocular injection of anti-VEGF for retinopathy of prematurity.
STRABISMUS
The Convergence Insufficiency Treatment Trial Group is a large, NEI/NIH supported and productive, multicenter, cross-discipline collaboration. Their random controlled trials (RCTs) have shown effective treatment of strabismus (convergence insufficiency) using orthoptic vision therapy.14-16
CATARACTS
IOL implantation, usually with an anterior vitrectomy, has become standard of care in the visual rehabilitation of children over the age of 1 year.17-19
The Infant Aphakia Treatment Trial, an NEI-sponsored multicenter collaboration, has produced data promoting standard of care treatment for infants with congenital unilateral cataracts. They found it better to leave infants under 7 months of age aphakic and place a contact lens (CL) rather than an IOL; they found no difference in visual acuity between the CL and IOL cohorts at 1 year of age. At 4.5 years, however, twice as many eyes in the CL cohort vs the IOL group had visual acuity>20/40.20,21 The IOL group had a 70% chance of needing a reoperation (most commonly due to visual axis opacification), but only 20% in the CL cohort required reoperation. The IOL was not found to be protective against secondary glaucoma.
OCULAR MOTILITY
The Active Pulley hypothesis
The traditional model of extraocular muscle (EOM) action was understood as following a fixed path from its insertion to its point of tangency with the globe, and then, a straight path to its origin in the orbital apex. Miller, Demer and Clark were instrumental in discovering that EOMs have associated functional connective tissue called “pulleys.” It is now believed that the orbital layer of each rectus EOM inserts onto a corresponding pulley, rather than on the globe.22 Only the global layer of the EOM inserts on the sclera.
The “active pulley hypothesis” proposes that rectus and inferior oblique pulleys are actively controlled by the action of the EOM’s orbital layers.23 This arrangement mechanically accounts for several aspects of normal ocular motor control, including Listing’s law and the vestibulo-ocular reflex. Further, pathology of the pulley system has been associated with predictable patterns of strabismus promoting unique surgical treatments.24
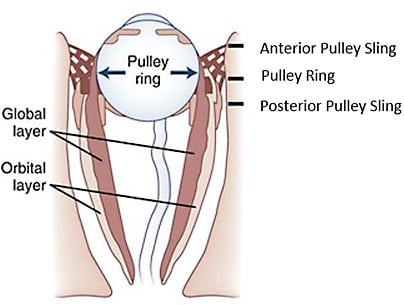
Figure 2. Diagrammatic representation of the structure of orbital connective tissues and their relationship to the fiber layers of the rectus extraocular muscles.
Credit: Redrawn from Demer, J.L., 2002. The orbital pulley system: a revolution in concepts of orbital anatomy. Ann N Y Acad Sci 956, 17-32.
“Chemical” resection-recession
Recent studies attempting to understand known toxicity of local anesthetics on eye muscles have demonstrated that bupivacaine (BUP) injected into EOMs induces a cycle of myotoxicity, degeneration, regeneration and hypertrophy of muscle fibers without adverse effects on other tissues. Scott et al, based on their work with both BUP and Botox (OnabotulinumtoxinA, Allergan), proposed combining injection of a horizontal rectus with BUP (resection) with antagonist injection of Botox (recession) to treat strabismus.25 They and others have demonstrated that strabismic alignment correction can be achieved using BUP plus Botox, thus paving the way for an increasing use of chemical resection/recession as an alternative to traditional eye muscle surgery.26
Congenital cranial dysinnervation disorders (CCDD)
CCDD encompasses several related non-progressive, genetic conditions caused by developmental abnormalities of cranial nerves/nuclei resulting in dysinnervation. CCDDs can be divided into three categories:
- Those that result in vertical ocular motility defects from dysinnervation of oculomotor and trochlear nerves and/or nuclei (eg, congenital fibrosis of the extraocular muscles and congenital ptosis);
- Those that result in horizontal ocular motility defects from dysinnervation of the abducens nerve and/or nucleus (eg, Duane Syndrome);
- Those that result from dysinnervation of the facial nerve and/or nucleus (eg, familial horizontal gaze palsy with progressive scoliosis, Marcus Gunn jaw wink (Figure 3) and Mobius).27
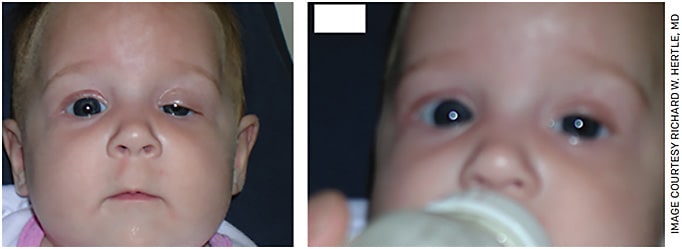
Figure 3. “Marcus-Gunn Jaw-Wink” in patient’s left eye.
The dedicated work by Engle and colleagues have demonstrated several CCDD genes (eg, CHN1, SALL4, KIF21A, PHOX2A, TUBB3) that have enhanced our understanding of the mechanisms involved in brain stem development and axonal guidance.28

Figure 4. “Duane Syndrome” in patient’s left eye.

Figure 5. “Double Elevatior Palsy” in patient’s left eye.

Figure 6. “Brown Syndrome” in patient’s left eye.

Figure 7. Congenital fibrosis of the extraocular muscles.
Nystagmus surgery and eye muscle proprioception
Through studies and research during the last 15 years, we have found that standard eye muscle surgery in children and adults with infantile nystagmus syndrome (INS) results in significant improvements in nystagmus intensity, null zone, waveform characteristics, best corrected optotype acuity, gaze dependent visual acuity, contrast sensitivity, visual recognition time and quality of life.29,30 These improvements are related to the surgical procedure and occur whether eye muscles are recessed, resected, transposed or detached and then reattached at the original insertion.
Recent neuroanatomical and neurophysiological discoveries support the hypothesis that disruption of newly discovered proprioceptive nerve endings in the EOM enthesis is the mechanism for INS damping after eye muscle surgery. This increases the indication for eye muscle surgery in patients with INS and creating new modeling of ocular motor pathways.31
THYROID EYE DISEASE (TED)
The FDA approval of Tepezza (teprotumumab, Horizon Therapeutics) for the treatment of TED in adults may eventually replace the need for major orbital surgery, radiation or oral steroids.32 Tepezza is a human-derived monoclonal antibody against IGF1-R, effectively blocking the responses of IGF1-R on orbital fibroblasts and reducing the inflammatory consequences of TED, such as chronic fibrosis and eyelid, ocular surface and optic nerve damage.
MINIMALLY INVASIVE STRABISMUS SURGERY
In 2007, Mojon, using a microscope, modified the fornix incision describing a technique to perform eye muscle surgery through 2-3 mm keyhole openings adjacent to the insertion. This technique theoretically decreases tissue trauma, surgical time, bleeding and healing time and improves patient comfort and visual rehabilitation.33
RETINA
Retinoblastoma is the most common primary intraocular malignancy of childhood and accounts for 10-15% of cancers in infancy. Treatment modalities have expanded in the last 25 years and now include intravenous, intra-ophthalmic arterial, intravitreal and intracameral chemotherapy.34 New consolidation therapies (cryotherapy and transpupillary thermotherapy) plus radiation-based therapies (external beam radiotherapy and plaque radiotherapy) have resulted in new protocols further preserving and restoring vision and salvaging the globe.35
Hereditary, genetic and metabolic diseases of the retina were once without a hope of treatment. Now, due to advances in molecular biology and genetic therapeutics and their translational application involving innovative anterior and posterior segment surgery, genetic and pluripotential cell transfer techniques are no longer science fiction.
Specific, targeted genetic treatment of many visual system diseases will become routine within the next decade.36
MYOPIA
Myopia has emerged as a serious public health issue and is now believed to be due to a complex combination of genetic and environmental factors with increased near work being predominant. Myopia prevalence reached 52.7% in 2020 among Chinese adolescents, which prompted the Chinese government to implement nationwide myopia control policies, including increasing the engagement of children in outdoor activities. Results from 12 RCTs and 15 cohort studies confirm that there is significantly less myopia progression and slower axial elongation when using topical atropine with effectiveness consistently related to dosing.37
CONCLUSION
In spite of the advances made in the diagnosis, treatment and understanding of visual system diseases in infant and children, I believe that access to care is the greatest challenge in the next 25 years. Of the millions of children in the United States entering school each year, less than 10% a year have had their visual systems checked. This is in part due to a lack of health insurance in >15%.37
It may be that the only ways the growing population of children can access eye care are through changes in renumeration, an increase in and expansion of eye-care provider type (eg, advance practice providers) and improved methods of screening for visual system diseases. I believe the current generation of professionals are up to this challenge. OM
REFERENCES
- Tdf. At the Crossings: Pediatric Ophthalmology and Strabismus Proceedings of the 52nd Annual Symposium of the New Orleans Academy of Ophthalmology, New Orleans, LA, USA, February 14 16, 2003: Robert J. Balkan, George S. Ellis Jr., and H. Sprague Eustis, Editors The Hague/The Netherlands, Kugler Publications, 2004, $125.00, 313 pages, 131 figures. Am Orthopt J. 2004;54:165-166.
- Beck RW. Clinical research in pediatric ophthalmology: the Pediatric Eye Disease Investigator Group. Curr Opin Ophthalmol. 2002;13:337-340.
- Wallace DK, Kraker RT, Freedman SF, et al. Short-term Outcomes After Very Low-Dose Intravitreous Bevacizumab for Retinopathy of Prematurity. JAMA Ophthalmol. 2020;138:698-701.
- Repka MX, Chandler DL, Holmes JM, et al. The Relationship of Age and Other Baseline Factors to Outcome of Initial Surgery for Intermittent Exotropia. Am J Ophthalmol. 2020;212:153-161.
- Freedman SF, Kraker RT, Repka MX, et al. Incidence and Management of Glaucoma or Glaucoma Suspect in the First Year After Pediatric Lensectomy. JAMA Ophthalmol 2020;138:71-5.
- Holmes JM, Kulp MT, Dean TW, et al. A Randomized Clinical Trial of Immediate Versus Delayed Glasses for Moderate Hyperopia in Children 3 to 5 Years of Age. Am J Ophthalmol. 2019;208:145-159.
- Pediatric Eye Disease Investigator Group, Holmes JM, Manny RE, et al. A Randomized Trial of Binocular Dig Rush Game Treatment for Amblyopia in Children Aged 7 to 12 Years. Ophthalmology. 2019;126(3):456-466.
- Shulman JP, Hartnett ME. Pharmacotherapy and ROP: Going Back to the Basics. Asia Pac J Ophthalmol (Phila). 2018;7:130-135.
- Sankar MJ, Sankar J, Chandra P. Anti-vascular endothelial growth factor (VEGF) drugs for treatment of retinopathy of prematurity. Cochrane Database Syst Rev. 2018;1(1):CD009734. Published 2018 Jan 8.
- Suelves AM, Shulman JP. Current screening and treatments in retinopathy of prematurity in the US. Eye Brain. 2016;8:37-43.
- Shah PK, Prabhu V, Ranjan R, Narendran V, Kalpana N. Retinopathy of Prematurity: Clinical Features, Classification, Natural History, Management and Outcome. Indian Pediatr. 2016;53 Suppl 2:S118-S122.
- Chiang MF, Quinn GE, Fielder AR, et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology. 2021;128:e51-e68.
- Daniel E, Quinn GE, Hildebrand PL, et al. Validated System for Centralized Grading of Retinopathy of Prematurity: Telemedicine Approaches to Evaluating Acute-Phase Retinopathy of Prematurity (e-ROP) Study. JAMA Ophthalmol. 2015;133:675-682.
- Convergence Insufficiency Treatment Trial Study G. Randomized clinical trial of treatments for symptomatic convergence insufficiency in children. Arch Ophthalmol. 2008;126:1336-1349.
- Convergence Insufficiency Treatment Trial Study G. The convergence insufficiency treatment trial: design, methods, and baseline data. Ophthalmic Epidemiol. 2008;15:24-36.
- CITT-ART Investigator Group. Treatment of Symptomatic Convergence Insufficiency in Children Enrolled in the Convergence Insufficiency Treatment Trial-Attention & Reading Trial: A Randomized Clinical Trial. Optom Vis Sci. 2019;96(11):825-835.
- Bremond-Gignac D, Daruich A, Robert MP, Valleix S. Recent developments in the management of congenital cataract. Ann Transl Med. 2020;8:1545.
- Bothun ED, Wilson ME, Vanderveen DK, et al. Outcomes of Bilateral Cataracts Removed in Infants 1 to 7 Months of Age Using the Toddler Aphakia and Pseudophakia Treatment Study Registry. Ophthalmology. 2020;127:501-510.
- Tadros D, Trivedi RH, Wilson ME. Primary versus secondary IOL implantation following removal of infantile unilateral congenital cataract: outcomes after at least 5 years. J AAPOS. 2016;20:25-29.
- Infant Aphakia Treatment Study G, Lambert SR, Buckley EG, et al. A randomized clinical trial comparing contact lens with intraocular lens correction of monocular aphakia during infancy: grating acuity and adverse events at age 1 year. Arch Ophthalmol. 2010;128:810-818.
- Infant Aphakia Treatment Study Group, Lambert SR, Lynn MJ, et al. Comparison of contact lens and intraocular lens correction of monocular aphakia during infancy: a randomized clinical trial of HOTV optotype acuity at age 4.5 years and clinical findings at age 5 years. JAMA Ophthalmol. 2014;132:676-682.
- Demer JL, Miller JM, Poukens V, Vinters HV, Glasgow BJ. Evidence for fibromuscular pulleys of the recti extraocular muscles. Invest Ophthalmol Vis Sci. 1995;36:1125-1136.
- Clark RA, Miller JM, Demer JL. Three-dimensional location of human rectus pulleys by path inflections in secondary gaze positions. Invest Ophthalmol Vis Sci. 2000;41:3787-3797.
- Miller JM. EOM Pulleys and Sequelae: A Critical Review. Invest Ophthalmol Vis Sci. 2019;60:5052-5058.
- Scott AB, Miller JM, Shieh KR. Treating strabismus by injecting the agonist muscle with bupivacaine and the antagonist with botulinum toxin. Trans Am Ophthalmol Soc. 2009;107:104-109.
- Josephson M, Mathias SA. Treatment of Intermittent Exotropia of the Convergence Insufficiency Type with Bupivacaine 0.75%: 5-Year Experience and Outcomes. J Binocul Vis Ocul Motil. 2019;69:3-7.
- Bosley TM, Abu-Amero KK, Oystreck DT. Congenital cranial dysinnervation disorders: a concept in evolution. Curr Opin Ophthalmol. 2013;24:398-406.
- Engle EC. The genetic basis of complex strabismus. Pediatr Res. 2006;59:343-348.
- Hertle RW, Dell'Osso LF, FitzGibbon EJ, Thompson D, Yang D, Mellow SD. Horizontal rectus tenotomy in patients with congenital nystagmus: results in 10 adults. Ophthalmology 2003;110:2097-2105.
- Hertle RW, Dell'Osso LF, FitzGibbon EJ, Yang D, Mellow SD. Horizontal rectus muscle tenotomy in children with infantile nystagmus syndrome: a pilot study. J AAPOS. 2004;8:539-548.
- Hertle RW, Chan CC, Galita DA, Maybodi M, Crawford MA. Neuroanatomy of the extraocular muscle tendon enthesis in macaque, normal human, and patients with congenital nystagmus. J AAPOS. 2002;6:319-327.
- Ali F, Chorsiya A, Anjum V, Ali A. Teprotumumab (Tepezza): from the discovery and development of medicines to USFDA approval for active thyroid eye disease (TED) treatment. Int Ophthalmol. 2021;41:1549-1561.
- Mojon DS. Review: minimally invasive strabismus surgery. Eye (Lond). 2015;29:225-233.
- Shields CL, Shields JA. Intra-arterial Chemotherapy for Retinoblastoma. JAMA Ophthalmol. 2016;134:1201.
- Ancona-Lezama D, Dalvin LA, Shields CL. Modern treatment of retinoblastoma: A 2020 review. Indian J Ophthalmol. 2020;68:2356-2365.
- Benati D, Patrizi C, Recchia A. Gene editing prospects for treating inherited retinal diseases. J Med Genet. 2020;57:437
- Gan J, Li SM, Wu S, et al. Varying Dose of Atropine in Slowing Myopia Progression in Children Over Different Follow-Up Periods by Meta-Analysis. Front Med (Lausanne). 2022;8:756398. Published 2022 Jan 13.
