







When one of my patients suffered ocular trauma that dislocated her toric lens, I asked the retina surgeon tasked with removing the lens to look at the topography I provided and choose an incision site on the steep axis to try to improve her refractive outcome. If the incision was placed on the flat axis, the incision would compound the astigmatism, but, if thoughtfully placed, the patient hopefully would have a better refractive outcome.
I apply the same care and attention to glaucoma surgery after LASIK or cataract surgery. There is a refractive emphasis to my practice — I want to get patients as close to spectacle-free as possible through refractive or cataract surgery. I also want to keep my patients happy long term. If they develop glaucoma 10 or 20 years down the road, I want them to be able to maintain their refractive gains.
I found that to be impossible with more traditional glaucoma surgeries, but now I find it more routine using the following approach.
MIGS REDUCE SURGICAL IMPACT ON VISION
Thankfully, we have many MIGS options to help us minimize drops and slow progression of glaucoma. Unlike traditional trabeculectomy and tube shunt surgeries, which affect refractive outcomes, many MIGS options have little or no effect on vision. Because the incisions are so small and we can select incision locations based on the patient’s topographic data, most MIGS do not substantially affect a patient’s refractive status. This is particularly true for MIGS options for mild to moderate glaucoma, including those used during cataract surgery.
I often combine MIGS during cataract surgery to manage glaucoma and hopefully limit progression. Typically reserved for mild to moderate glaucoma, trabecular micro-bypass with the Hydrus (Ivantis) or iStent (Glaukos) has little or no effect on refraction. The same could be said of goniotomy or canaloplasty. Other options may be considered in severe glaucoma and sometimes in combination, such as goniotomy with the Kahook Dual Blade (New World Medical) or the TrabEx device (MST), or ab interno viscodilation of the canal with or without goniotomy, including the OMNI Surgical System (Sight Sciences) and ABiC with iTrack (Nova Eye Medical).
In some cases, when I believe canal surgery will be of too little benefit, I think of subconjunctival filtration with the XEN Gel Stent (Allergan). The Preserflo Microshunt (Santen) may prove to have good refractive outcomes similar to XEN, once it is available in the months ahead.
SEVERE GLAUCOMA AFTER REFRACTIVE SURGERY
Traditionally, when a patient had severe glaucoma and we ruled out canal surgery, the next step has been trabeculectomy or tube shunt, but trabs and tubes can significantly alter refractive status. The surgical approach for trabs and tubes can induce significant astigmatism and a shift toward hyperopia.1-5
Imagine the disappointment of patients in a cataract and refractive practice like mine, where many paid for LASIK or an upgraded advanced technology lens implant 15 to 20 years ago and now have developed another condition. If they fail conservative treatments, some of the more traditional surgical options that may be indicated will likely undo the refractive improvements they have become accustomed to.
This problem is particularly difficult for patients with presbyopia-correcting IOLs. Surgeons screen patients for glaucoma before cataract surgery, and the disease may impact not only the addition of a concurrent MIGS procedure but also patients’ suitability for presbyopia-correcting IOLs. Glaucoma development and progression is age-related, however, so the disease is not always evident at the time of surgery. Some patients with presbyopia-correcting IOLs develop glaucoma 10 to 15 years down the road.
The question is, “What do we do now?” We can add glaucoma drops, which also can make patients unhappy. Issues such as ocular surface redness, discomfort and the refractive problems associated with poor quality tear film are well known. More importantly, drops often are not enough. We opt for a trab or tube in advanced cases, but, as mentioned before, this often changes the patient’s refractive status. Alternatively, I prefer an option that controls pressure with less risk of inducing refractive changes.
PRESERVING REFRACTIVE RESULTS
When I talk to colleagues about induced refractive errors from trabs and tubes, particularly with an eye toward retaining refractive outcomes for my previous LASIK and premium cataract patients, I often hear, “What do you expect? The patient has severe glaucoma — everything else is out the window.” I understand this response. Indeed, it is better to control glaucoma and suffer a change in refraction than to lose vision from this incurable disease. But I don’t believe it is true that “everything else is out the window.” I don’t believe the two are mutually exclusive. A patients’ refractive status does not have to worsen when treating glaucoma.
To maintain patients’ happiness with LASIK and premium IOL surgery after they’ve developed severe glaucoma, I began using the XEN Gel Stent 4 years ago for the large majority of cases where I would have performed trabeculectomy in the past. In fact, I used to do 30 trabs a year, but I’ve only done two in the last 2 years. I have been delighted with the XEN, not just because it is less invasive6 and has a lower risk of complications,7 but also because it generally has minimal effect on refraction.8
In moderate and advanced glaucoma, XEN can keep my patients happy — it minimizes drop burden, improves their ocular surface health and improves glaucoma control with minimal impact on the refractive result. I continue to choose trab for cases where XEN contraindications exist, such as conjunctival disease or scarring at the implant site and active inflammation.
XEN drains aqueous into the subconjunctival space. Techniques for the procedure have evolved over the years to optimize the outcomes. XEN was originally an ab interno procedure, but now many have adapted an ab externo approach that is off-label. I use the latter, which requires a few minutes to implant the stent. Like trabeculectomy, XEN requires the use of mitomycin C and is a bleb-forming procedure.
XEN blebs tend to be flatter than those for trabeculectomy,9 but bleb management is more likely to require needling.10 With refinements in technique, my needling rate is less than 10%.
From my patients’ perspective, surgery is quick and easy. They see well immediately and return to their baseline vision in 1 or 2 days. I let them resume normal activities as soon as they leave the surgery center. They see me again the next day, then again at 4 to 6 weeks. What patients don’t realize is that if they’d had trab or tube — the other common surgical options at this point in their disease — they would likely have a shift in their refractive status and be back in glasses, and they would have twice the number of follow-up visits and greater potential for complications.
It is still possible for patients to require additional surgery later as the disease progresses, and XEN does not preclude having another procedure. In many cases, before going to trabeculectomy, I will use another XEN or two to preserve vision and help patients reduce the need for topical medications.
CASE EXAMPLE
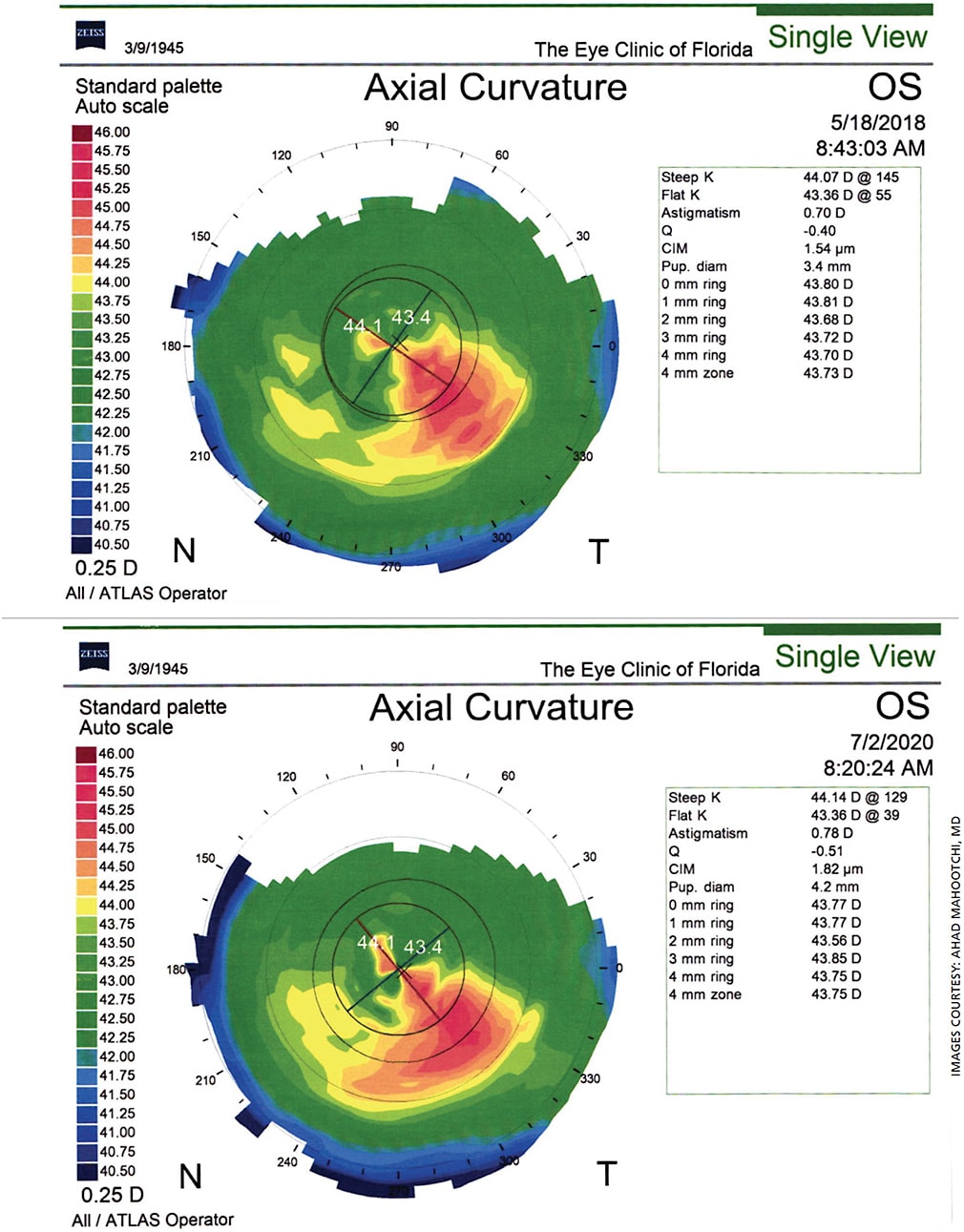
In a recent case, a patient who had cataract surgery with a multifocal IOL in 2008, eliminating the need for eyeglasses, was diagnosed with glaucoma in 2019 at age 76. She was prescribed two medications, but they only lowered her pressures to 20 mm Hg OS and 23 mm Hg OD (still too high), and the combination of drops was very hard on her ocular surface. She was referred back to me for possible trabeculectomy. She was a good candidate for XEN, so we chose that option instead.
After surgery, the patient went golfing with her friends the same day. One month postop, her IOP was 15 mm Hg OU. Her eyes were no longer red, and she was still very happy with her vision (Figure). Before XEN was available, I would have had to perform a trab or tube on this patient. Even if all went well, she would have had a longer recovery and needed eyeglasses. Now when we manage the glaucoma with this technology, we don’t have to create a new set of problems, and patients can often retain the results from their prior LASIK or premium lens surgery. OM
REFERENCES
- Claridge KG, Galbraith JK, Karmel V, Bates AK. The effect of trabeculectomy on refraction, keratometry and corneal topography. Eye (Lond). 1995;9:292-298.
- Kook MS, Kim HB, Lee SU. Short-term effect of mitomycin-C augmented trabeculectomy on axial length and corneal astigmatism. J Cataract Refract Surg. 2001;27:518-523.
- Kim GA, Lee SH, Lee SY, et al. Surgically induced astigmatism following trabeculectomy. Eye (Lond). 2018;32:1265-1270.
- Alvani A, Pakravan M, Esfandiari H, et al. Ocular biometric changes after trabeculectomy. J Ophthalmic Vis Res. 2016;11:296-303.
- Nasrabadi FD, Hashemi H, Amiri MA, et al. Evaluation of Changes in Refractive Errors Before and After Trabeculectomy and Shunt Surgery. Clin Optom (Auckl). 2020;12:107-112.
- Olgun A, Duzgun E, Yildiz AM, et al. XEN Gel Stent versus trabeculectomy: Short-term effects on corneal endothelial cells. Eur J Ophthalmol. 2021;31:346-353.
- Theilig T, Rehak M, Busch C, et al. Comparing the efficacy of trabeculectomy and XEN gel microstent implantation for the treatment of primary open-angle glaucoma: a retrospective monocentric comparative cohort study. Sci Rep. 2020;10:19337.
- Lenzhofer M, Strohmaier C, Hohensinn M, et al. Change in visual acuity 12 and 24 months after transscleral ab interno glaucoma gel stent implantation with adjunctive Mitomycin C. Graefes Arch Clin Exp Ophthalmol. 2019;257:2707-2715.
- Teus MA, Moreno-Arrones JP, Castaño B, et al. Optical coherence tomography analysis of filtering blebs after long-term, functioning trabeculectomy and XEN stent implant. Graefes Arch Clin Exp Ophthalmol. 2019;257:1005-1011.
- Sharpe R, Pham G, Chang P. Comparison of ab interno XEN gelatin stent vs trabeculectomy with mitomycin C: A retrospective study. J Curr Glaucoma Pract. 2020;14:87-92.
About the Author
