







Optical coherence tomographic angiography (OCTA) is becoming a clinical standard for a variety of retinal diseases. In some cases, it may even illustrate pathology better than standard imaging, such as OCT or dye angiography.
This article is an overview of this technology and how it can be best utilized in practice.
OCTA OVERVIEW
OCTA detects and illustrates movement in ocular structures in the posterior segment of the eye using OCT technology, in which sequential OCT B-scans are acquired. Any change between these scans is considered movement. For the most part, the only moving structure in the posterior segment is blood and its particles. The variation in the phase and/or the intensity of the backscattered light is then determined based on the comparison of the multiple B-scans in each section.
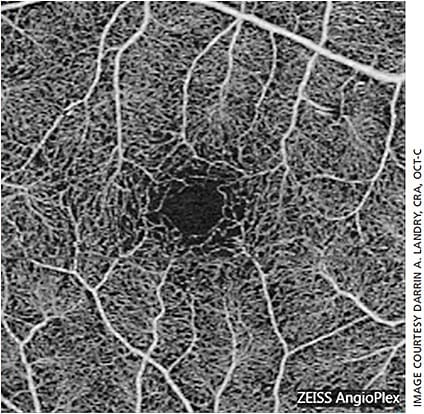
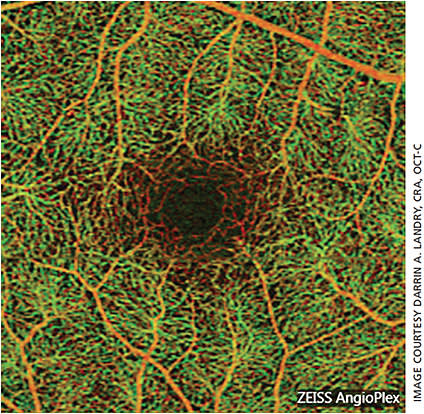
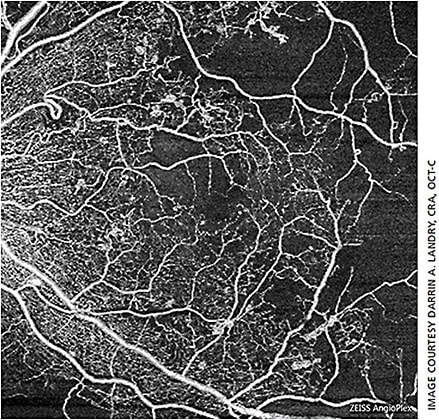
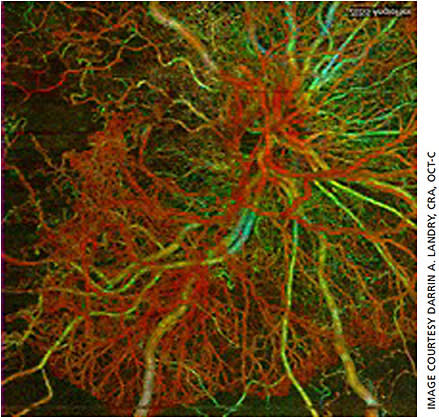
Because the particles moving in blood cause the most variation in the phase and intensity of backscattered light, blood vessels appear brightest on OCTA images and static tissue (retinal structures, nonmoving structures) appear dark. The resulting image closely mimics an early fluorescein angiogram, as vascularity is illustrated in white (or false color — pseudo color is applied to the image to illustrate the different depths of vasculature) (Figures 1 and 2). The important difference between OCT and OCTA: OCT images anatomical structure, while OCTA images vascular structure.1
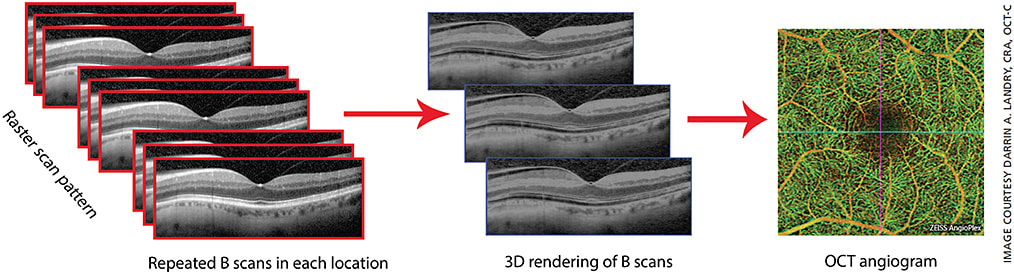
OCTA utilizes OCT technology, which scans in the X and Y axes. OCTA also scans in the Z axis, allowing for imaging “en face,” which is similar to how we image posterior pole color and dye angiography. Using en-face imaging, the OCTA images multiple layers from the anterior retina to the choroid (Figure 3).1
Three spectral domain-OCTA systems are commercially available in the United States: Heidelberg Spectralis, Optovue Angiovue and Zeiss Angioplex. Also, the Zeiss Plex Elite is a swept-source OCTA system available in the United States.
SEGMENTATIONS
OCTA software typically divides retinal layers into the following vascular segmentations:
- Superficial retinal vasculature. This structure is the innermost vascular layer of the retina and is what we visualize when viewing fundus photographs or fluorescein angiography. This vascular layer consists of large retinal vessels and the smaller capillaries that make up the foveal avascular zone. Consisting of the capillary vascular plexus we see on fluorescein angiography, this layer is located within the ganglion cell layer, which, along with the deep retinal plexus, makes up the vascularity in the neurosensory retina.2
- Deep retinal plexus. Connected to the superficial retinal vasculature by perpendicular vessels,3 the deep retinal plexus outer border is defined by the inner nuclear layer. Before OCTA, we had not been able to image this vascular structure with standard angiography, as the fluorescence from the superficial vasculature blocks any fluorescence from the deep retinal plexus. With OCTA, we can view the vascular structure independently without the interference or blockage of the superficial retinal vasculature.
- Avascular layer. This layer is defined as the area between the outer plexiform layer in the inner border and the ellipsoid zone or Bruch’s membrane in the outer border.4 In the absence of disease, this area is void of vasculature; however, when neovascularization forms, typically from exudative macular degeneration, the source of these neovascular membranes may start in the choroid and proliferate through a break in Bruch’s membrane. The resulting neovascularization would be identifiable in the avascular layer on OCTA.
- Choriocapillaris. This layer refers to the smaller choroidal vessels found under Bruch’s membrane. Neovascular membranes from exudative macular degeneration may be isolated in this layer by OCTA, and the source of that membrane may also be identifiable in the choriocapillaris.1
- Choroid. The larger choroidal vessels make up this layer, which extends posteriorly to the sclera. Due to the nature of OCTA technology, the light used to image is scattered and attenuated by the retinal pigment epithelium (RPE) and the choriocapillaris, above the choroid, which reduces the ability to image choroidal vessels.
UTILIZING OCTA IN PRACTICE
Imaging in the Z axis gives us the ability to determine the depth of vasculature structure, allowing the clinician to determine which anatomical layer the active vessels are in. Understanding the underlying retinal disease helps to guide the imager on the layer most important.
For instance, diabetic retinopathy can result in impaired perfusion, microaneurysms and neovascularization. These changes are best illustrated in the superficial and deep retinal vascular layers. For exudative choroidal neovascularization, most of the pathological structures lie under the retina and RPE. Also, in some cases, such as retinal angiomatous proliferation lesions, intraretinal vascular changes can be found.
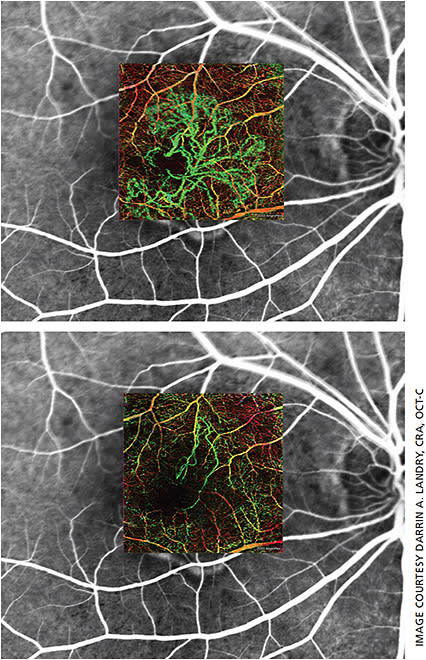
Most OCTA systems take only seconds to acquire images, so repeated scans at follow-ups can help in tracking the progression of a disease or to monitor changes related to treatment (Figure 4). After initial OCT scans are acquired, the imager may determine that an OCTA is justified. For instance, in a patient with subretinal or sub-RPE fluid, the presence of a neovascular membrane is likely. Therefore, the imager can acquire OCTA scans following the OCT, giving the clinician much more data. Any disease or pathology that involves the retinal or choroidal vascular system would benefit from an OCTA scan.
At this time, there are no reimbursement codes specifically for OCTA, but, as it utilizes OCT technology, it is reasonable to bill as an OCT.
We are still in the pioneering stage of OCTA, and therefore rules are very fluid. The best rule of thumb initially is to scan every patient; however, the imager will realize which pathologies are best presented on OCTA over time.
With the ability to visualize every functioning capillary, OCTA can be used in place of standard dye angiography for some pathologies. Without the ability to measure or quantitate blood flow, dye angiography will still be the clinical standard until advanced OCTA analytics are available. OM
REFERENCES
- Landry DA, Kashani AH. OCT and OCT Angiography, Clinical Reference and Case Studies. Bryson Taylor Publishing; 2017
- Novalis E, Baumal C. The clinical utility of OCT angiography: Rev Ophthal. January 10, 2017.
- Bonini Filho MA, Adhi M, de Carlo TE, et al. Optical coherence tomography angiography in retinal artery occlusion. Retina. 2015; 35:2339-2346.
- Turgut B. The importance of VRI and AOR segmentations in optical coherence tomography angiography. Adv Ophthalmol Vis Syst. 2017;6:00199.
About the Author
