







Whether working around the house or yard or on a craft you enjoy, the right tools almost always lead to the best results. The same holds true for diagnosing retinal issues, as the right tools can provide you the best chance to maintain and save your patients’ vision.
Early detection is key to preserving vision. For instance, MARINA and ANCHOR studies revealed that the more early or immature a choroidal neovascularization (CNV) lesion is, the better final visual acuity outcome is expected after treatment, according to a 2015 literature review in the International Journal of Retina and Vitreous.
Here, you’ll learn about major advances in retina diagnostic tools: ultra-widefield fundus photography, optical coherence tomography angiography (OCTA) and telemedicine.
WIDER VIEW
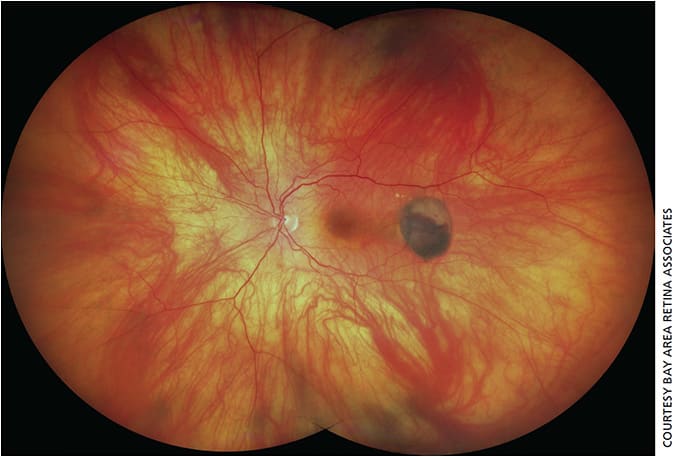
Conventional fundus photography, with roughly 60° of capture, allows you to see less than half of the retina’s entire field. Ultra-widefield fundus photography, by contrast, allows you to capture up to 200° in a single image, without any additional manipulation such as creating a montage (Figure 1, page 36).
This ability has “revolutionized” the profession, says Shlomit Schaal, MD, PhD, professor and chair of the department of ophthalmology and visual sciences at the University of Massachusetts Medical School, Worcester, Mass. The technology represents an easy way to capture the periphery of the retina and “to alert the physician that there is a pathology there,” says Dr. Schaal.
Manjot K. Gill, MD, associate professor of ophthalmology and director of vitreoretinal fellowships at Northwestern University Feinberg School of Medicine, Chicago, credits ultra-widefield fundus photography, in conjunction with fluorescein angiography, with changing her approach to diabetic retinopathy patients. “On a daily basis, I’m using this to guide my management of diabetic patients,” Dr. Gill says. The ability to capture up to 200° of the retina in a single image allows her to detect the extent of diabetic changes and then follow those changes longitudinally.
Dr. Gill has used this technology, in this case a California system (Optos), routinely for about a year and says it allows her to examine areas of the retina that could not be otherwise imaged by conventional photography, so she can better understand the extent of a patient’s diabetic pathology. Depending on her findings, it helps guide her decisions about treating a patient or following the patient more closely. For patients with conditions like a retinal tear in the periphery or a retinal detachment, Dr. Schaal can use the widefield images to show patients their surgery results.
While a major ophthalmic tool, Dr. Gill points to false color representation and eyelash artifact as two areas that can be improved. And there is a learning curve: “You have to become familiar with viewing these images and be careful not to over-interpret them and look beyond the artifacts,” she says. (For more on ultra-widefield imaging, see “Screening with widefield fundus photography” in our July issue, page 38, or at https://tinyurl.com/y59835ud .)
OCT ADVANCES
OCT remains the mainstay in diagnosing retinal problems. Vendors continue to improve this technology, and the trend has been “faster devices that allow you to obtain more B-scan lines for denser scan patterns and oversampling,” says K. Bailey Freund, MD, Vitreous Retina Macula Consultants of New York and clinical professor, department of ophthalmology, NYU School of Medicine. This permits scanning the same part of the tissue several times and then averaging these scans to increase the signal-to-noise ratio, resulting in better detail and less artifact. At least one device has achieved 100,000 A-scans per second.
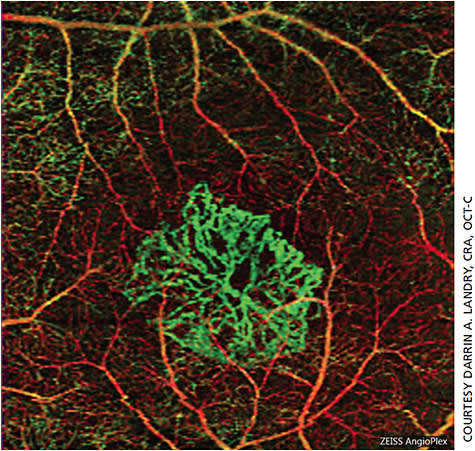
However, a great deal of excitement now centers on OCTA, which detects the movement of erythrocytes through blood vessels and produces a map of ocular blood flow (Figure 2). OCTA permits visualization not only of the superficial and middle layers of the retina, but also the deep capillary plexus.
“This is allowing us to elucidate different layers of vasculature in the retina and choroid that we could not otherwise capture with standard fluorescein angiography,” says Dr. Gill. It provides “tremendous insight into the pathogenesis of various disease entities, allowing us to characterize them in ways that we previously could not with fluorescein angiography.”
OCTA provides various advantages, including:
- Depth-resolved. Dye angiography doesn’t allow visualizing the deep vascular plexus, which is where much of the early damage occurs, particularly in diabetic retinopathy, Dr. Freund says.
- Noninvasive. This eliminates concerns about administering an injection and potential allergic reactions to dye, Dr. Gill says.
- Speed. Acquiring the image is much quicker (two to three minutes) compared to standard fluorescein angiography (20-30 minutes), Dr. Gill says.
OCTA, Dr. Freund says, can be useful for certain retinal vascular diseases, including diabetic retinopathy, retinal vein occlusion and arterial occlusion. For these diseases, a clinician wants to see potential damage to small capillaries that “may not always appear clearly on a fluorescein angiogram.”
Dr. Gill has found OCTA “extremely valuable” for managing AMD. “It allows you to visualize CNV without the inconvenience of an invasive test,” she adds. “In some instances, I have been able to detect subclinical neovascularization before it has started to cause visual symptoms. I may not necessarily treat these patients, but I will follow them very closely.”
For patients diagnosed with exudative macular degeneration, OCTA, says Dr. Gill, can help determine the location, morphology and response of the choroidal neovascular membrane to anti-VEGF therapy and in some cases may guide her treatment decision-making as to whether to continue anti-VEGF therapy.
What’s more, OCTA has “opened up a whole new area of great interest,” says Dr. Freund. Practitioners are aware, he says, that there are quite a few eyes that clinically appear to have non-neovascular AMD but harbor non-exudative Type 1 (sub-retinal pigment epithelium) CNV. “We believe that eyes with this finding are at an increased risk for conversion to a more active type” of neovascularization, he notes.
Nadia Waheed, MD, MPH, associate professor, Tufts University School of Medicine, Boston, and director of Boston Image Reading Center, uses OCTA to screen dry AMD patients for the presence of nonexudative subclinical CNV. These patients are at a higher risk for conversion to wet AMD, she says.
Although OCTA is no longer in its infancy, much remains to be learned about the technology and how it will be used in practice, notes Dr. Gill,. How this technology will be used in practice is still a question. We are “given these amazing images, but now we have to decide how to adopt them into our clinical practice and whether they will change our management,” she says.
Although a significant advance, OCTA is not without its limitations, including:
- Field of view. Generally, OCTA delivers images of the macular region. For retinal vascular disease, OCTA is good at looking at macular blood flow, says Dr. Freund. “But often, the devices can’t really do a as good a job of showing us the vascular detail once we go beyond a 6x6mm scan area.”
- Time needed for interpretation. With standard structural OCT, says Dr. Gill, point-to-point registration — comparing images taken at various times for a patient — is seamless and easy. For OCTA, this process can be more time-intensive to access and scroll through the images as well as interpret the images. With structural OCT, you might have a snapshot of the fovea, which you compare to a snapshot taken in a previous visit. With OCTA, she notes, viewing images is more cumbersome, especially when trying to compare images from different time points, Dr. Gill notes. You may also need to manually segment images to ensure you are viewing the appropriate layers of the retina and capture the pathology.
- Learning curve and artifacts. OCTA involves a fairly steep learning curve, says Dr. Freund, in part because of many potential artifacts. One of the most difficult of these, he says, is projection artifact, in which movement of blood cells within superficial retinal layers causes fluctuations in the light reaching deeper tissue; this can produce artifactual images of vessels in these deeper locations. However, he notes, manufacturers are getting better at removing some of these artifacts. It must be emphasized that misinterpretation of the OCTA can lead to inappropriate patient care. Although the OCTA will likely be a valuable tool and possibly a standard of care in the future, much work remains to be done.
GOING REMOTE
As with many health-care settings, ophthalmology can benefit from telemedicine (the use of technology to care for patients remotely). Current applications of telemedicine, says Dr. Schaal, include stroke and retinopathy of prematurity, for which nurses can take images of the fundus of babies in the neonatal intensive care unit and send the images to an ophthalmologist for interpretation.
For patients with high risk for conversion to neovascular AMD, such as those with multiple large drusen and focal hyperpigmentation, Dr. Freund often suggests the ForeseeHome monitoring device (Notal Vision). The goal is to detect visual disturbances that could indicate conversion from non-neovascular AMD to neovascular AMD so treatment can start earlier. The ForeseeHome, according to Notal Vision, is intended for use in the detection and characterization of central and paracentral metamorphopsia in AMD patients as an aid in monitoring progression of disease factors causing metamorphopsia, including CNV. It is intended for home use by patients with stable fixation.
For one of Dr. Freund’s patients, the use of ForeseeHome led to a much better outcome than if remote monitoring had not been available. The patient had converted to active exudation, but her vision had not been affected to the extent that she noticed it. Because of the test, the patient was told to come to the office. Had she noticed it, the patient said she would probably have gotten her glasses checked before realizing this could be a macular problem, Dr. Freund says. “So that was quite a save.”
While of assistance, the device is not perfect. It is detecting a visual change, which is not always correlated with the anatomic change of fluid or bleeding, says Dr. Freund. This can lead to false positives.
Another drawback to telemedicine, from a business perspective, involves payment levels. “The main hindrance for telemedicine right now is reimbursement,” says Dr. Schaal, who gives an example of reimbursement being much less for screening for diabetes in an eye exam done by telemedicine than in person. “But I believe that this is going to change.”
CONCLUSION
Whether it’s a wider view, a deeper map of retinal blood flow or remote monitoring patients, these technologies can help physicians provide optimal care. With these tools, ophthalmologists can do even more to protect and preserve their patients’ sight. OM