







But I’m already using so many drops … why do I have to use more?
This is an all-too-familiar question I am asked when I address a glaucoma patient’s signs and symptoms of dry eye or other forms of ocular surface disease (OSD). The management of dry eye in the glaucoma patient — or the management of glaucoma in a dry eye patient — can be daunting and frustrating. Both diseases have an increased prevalence with age, are chronic, and may be progressive without proper long-term or life-long management. And it is estimated that close to 50% of patients with glaucoma suffer from OSD. The difficulty we face is that our “conservative” management of glaucoma (topical medication) tends to worsen surface disease, while the management of OSD increases the patient’s medication burden and can be overwhelming to a patient and lead to confusion and increased noncompliance.
The Disruptive Nature of Glaucoma Medications
Tear film is composed of lipid, mucinous, and aqueous layers, which work in unison to ensure optimal function of the ocular surface. Ocular surface disease (OSD) is a multifactorial process resulting from dysfunction of tear film and its resulting inability to protect and sustain the health of the conjunctiva and cornea. OSD may manifest from a decrease in aqueous production, instability of the tear film, and/or ocular surface breakdown with may lead to the characteristic signs and symptoms of dry eye syndrome (DES).1 The incidence of DES in the general population is 3.9% to 9.8%, with that number on the higher end for females and those of advancing age.2,3
Treatment of dry eye can range from the use of artificial tears in mild cases to autologous serum in the most severe. The actual management of dry eye, like glaucoma, is tailored to the underlying etiology. In cases of aqueous tear deficiency, supplementation with lubricants can suffice, but some patients may require punctual occlusion or prescription medications like Restatsis (Allergan), which acts to suppress chronic inflammatory changes within the lacrimal glands or more recently, Xiidra (Shire) which mitigates the upregulation of inflammatory markers on the ocular surface, but true mechanism of action remains unclear. When lid margin disease is evident, addition of lid hygiene, oral tetracycline, or even Intense Pulsed Light Therapy (Lumenis) may be needed.
Our management of glaucoma directly influences the health of the ocular surface by inducing changes to the eye and ocular adnexa. Currently, lowering and maintaining intraocular pressure is the only method of controlling glaucoma.4 Although selective laser trabeculoplasty has increased in use as a primary therapy, topical anti-glaucoma medications are typically employed as the first-line IOP lowering treatment. Numerous studies have shown that topical glaucoma medications cause OSD. In one study, dry eye symptoms were present in 59% of patients using glaucoma medications, with 27% reporting severe symptoms. Signs were present in 78% of patients, respectively.5 Ghosh et al reported ocular surface disease in 70.3% of patients prescribed glaucoma medications for greater than 6 months (compared with 33% of controls).6 Interestingly, despite the higher prevalence of OSD in glaucoma patients, symptoms may not be as offensive to those undergoing glaucoma therapy as compared to the general population. One potential reason is the corneal neurotoxicity and reduced corneal and conjunctival sensitivity induced by chronic benzalkonium chloride application, a preservative used in many glaucoma medications.7,8
The reasons for the increased prevalence of OSD in glaucoma patients can be directly attributed to either the glaucoma medication’s active ingredient or its preservative. Benzalkonium chloride (BAK) is a quaternary ammonium cation, and one of the most commonly used preservatives in ophthalmology. As a detergent, this preservative nicely emulsifies fatty acids, which helps to denature proteins and the lipid bilayer on bacterial cell walls, preventing contamination in multidose bottles. This biochemical property, however, also disrupts the lipid layer of the tear film, leading to a pronounced evaporation and increased concentration of the aqueous component of the tear film. The newly hyperosmotic tear film then becomes cytotoxic to the surface epithelium.9,10 These responses have been found to be dose dependent and can also be seen in preservative-free formulations to a lesser extent.1
The lipid layer is directly affected by the deleterious effects medications have on the morphology and function of sebaceous cells. An obstructive form of meibomian gland dysfunction (MGD) may be present in up to 92% of patients treated with prostaglandin analog monotherapy.11 Similarly, timolol and pilocarpine may have direct negative effects on meibomian gland epithelial cells.12 Reduction or alteration of the production of sebum can exacerbate the changes to the lipid layer already adversely affected by BAK.
Next, topical glaucoma medications induce chronic inflammatory changes to the ocular surface resulting in a decrease in goblet cells population and increased numbers of inflammatory cells (macrophages, lymphocytes, mast cells, fibroblasts) within the conjunctival substantia propria.13 This chronic subclinical inflammation has wide-ranging consequences, including OSD, poor corneal wound healing, and increased failure rate of traditional glaucoma filtering surgeries.14-16 The reduction in goblet cells also leads to a decrease in mucin production, another vital component of the tear film.
Managing Patients With Combined Glaucoma and Ocular Surface Disease
Our standard first-line therapy for managing glaucoma is actuating another disease process. Above, we highlighted the contributions of topical glaucoma medications to OSD. It is important to decipher whether disruption of the homeostatic environment of the ocular surface is due to the active drug, the preservative, or both. Minimizing the offending agents can help prevent or minimize signs and symptoms of OSD. Namely, reducing the need for topical glaucoma medications or, at the very least, attempting to use drops with a less offensive preservative. Stabilized oxychloro complex (Purite; Bio-Cide International Inc.), used in conjunction with brimonidine (Alphagan; Allergan) 0.15%, is believed to reduce the incidence of allergy and hyperemia compared with BAK-brimonidine 0.2%.17 SofZia is the preservative system in Travatan Z (travoprost; Alcon Laboratories). Multiple studies have shown a favorable tolerability profile of SofZia.18 There is an increasing trend toward compounding glaucoma medications without the preservatives. Unfortunately, there are currently no studies that examine efficacy of these medications, as preservatives and pH of the solution play an important role in ocular solubility, penetrance, bioavailability, and, ultimately, efficacy.
When medications alone control patients’ IOP and a concomitant cataract is not present, selective laser trabeculoplasty (SLT) is a nice noninvasive, office-based method for reducing medication burden.19 Another noninvasive method for controlling IOP is the newly released micropulse laser by Iridex.20 This technology, however, requires retrobulbar anesthesia or a visit to the operating room to properly anesthetize the patient’s eye. When patients have uncontrolled glaucoma or concomitant cataracts, several incisional procedures exist to decrease or remove the burden of daily topical medication use. Minimally invasive glaucoma surgery (MIGS) has become important in reducing medication burden while minimizing the risks associated with conventional glaucoma filtering surgery (hyoptony, wound complications, choroidal effusions or hemorrhage, bleb-related infections, and so on).
The various MIGS devices and surgeries target different aspects of the traditional outflow system or aim to circumnavigate it altogether. Available procedures include bypassing the trabecular meshwork with iStent (Glaukos); viscodilating Schlemm canal and collector channels with Visco360 (Sight Sciences) or iTrack (Ellex); removing, ablating, or opening various amounts of trabecular meshwork with the Kahook Dual Blade (New World Medical), the Trabectome (NeoMedix), or iTrack; supraciliary stenting with Cypass (Alcon); and subconjuctival aqueous shunting with the Xen gel stent (Allergan).
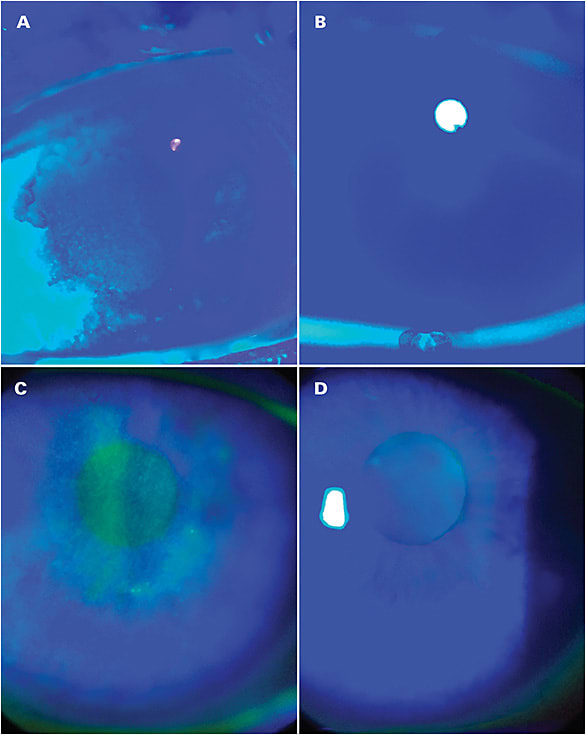
A great number of studies in the literature have examined all of these devices and consistently show IOP reduction and, maybe just as important, reduced need for topical medications. We have found that adding MIGS procedures to cataract surgery have drastically reduced or even eliminated the need for topical medications in a vast majority of patients. With our increased knowledge of how each device or procedure works, we are now tailoring treatment to each patient’s clinical profile to enhance efficacy, much like we tailor our dry eye management. These measures of reducing medication burden can improve a patient’s clinical picture from the signs of OSD to enhanced vision and overall quality of life (Figure 1). GP
References
- Ramili N, Supramaniam G, Samsudin A, Juana A, Zahari M, Choo MM. Ocular surface disease in glaucoma: effect of polypharmacy and preservatives. Optom Vis Sci. 2015;92(9):222-226.
- Schaumberg DA, Dana R, Buring JE, Sullivan DA. Prevalence of dry eye disease among US men: estimates from the Physicians’ Health Studies. Arch Ophthalmol. 2009;127(6):763-768.
- Schaumberg DA, Sullivan DA, Buring JE, Dana MR. Prevalence of dry eye syndrome among US women. Am J Ophthalmol. 2003;136(2):318-326.
- Heijl A, Leske C, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression. Arch Ophthalmol. 2002;120(10):1268-1279.
- Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17(5):350-355.
- Ghosh S, O’Hare F, Lamoureux E, Vajpayee RB, Crowston JG. Prevalence of signs and symptoms of ocular surface disease in individuals treated and not treated with glaucoma medication. Clin Exp Ophthalmol. 2012;40(7):675-681.
- Martone G, Frezzotti P, Tosi GM, et al. An in vivo confocal microscopy analysis of effects of topical antiglaucoma therapy with preservative on corneal innervation and morphology. Am J Ophthalmol. 2009;147(4):725-735.
- Benitez-Del-Castillo JM, Acosta MC, Wassfi MA, et al. Relation between corneal innervation with confocal microscopy and corneal sensitivity with noncontact esthesiometry in patients with dry eye. Invest Ophthalmol Vis Sci. 2007;48(1):173-181.
- Kaur IP, Lal S, Rana C, Kakkar S, Singh H. Ocular preservatives: associated risks and newer options. Cutan Ocul Toxicol. 2009;28(3):93-103.
- Kusano M, Uematsu M, Kumagami T, Sasaki H, Kitaoka T. Evaluation of acute corneal barrier change induced by topically applied preservatives using corneal transepithelial electric resistance in vivo. Cornea. 2010;29(1):80-85.
- Mocan MC, Uzunosmanoglu E, Kocabeyoglu S, et al. The association of chronic topical prostaglandin use with meibomian gland dysfunction. J Glaucoma. 2016;25(9):770-774.
- Zhang Y, Kam WR, Liu Y, Karakaya J, Irkec M. Influence of pilocarpine and timolol on human meibomian gland epithelial cells. Cornea. 2017 Jun;36(6):719-724.
- Broadway DC, Grierson I, O’Brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication. I. The conjunctival cell profile. Arch Ophthalmol. 1994;112(11):1437-1445.
- Broadway DC, Grierson I, O’Brien C, et al. Adverse effects of topical antiglaucoma medication. II. The outcome of filtration surgery. Arch Ophthalmol. 1994;112(11):1446-1454.
- Pinheiro R, Panfil C, Schrage N, Dutescu RM. The impact of glaucoma medications on corneal wound healing. J Glaucoma. 2016;25(1):122-127.
- Miki T, Naito T, Fujiwara M, et al. Effects of pre-surgical administration of prostaglandin analogs on the outcome of trabectulectomy. PLoS One. 2017;12(7):e0181550.
- Katz LJ. Twelve-month evaluation of brimonidine-purite versus brimonidine in patients with glaucoma or ocular hypertension. J Glaucoma. 2002;11(2):119-126.
- Lewis RA, Katz GJ, Weiss MJ, et al. Travoprost 0.004% with and without benzalkonium chloride: a comparison of safety and efficacy. J Glaucoma. 2007;16(1):98-103.
- Nagar M, Ogunyomade A, O’Brart DP, Howes F, Marshall J. A randomised, prospective study comparing selective laser trabeculoplasty with latanoprost for the control of intraocular pressure in ocular hypertension and open angle glaucoma. Br J Ophthalmol. 2005;89:1413-1417.
- Gavris M, Olteanu I, Kantor E, Mateescu R, Belicioiu R. IRIDEX Micropulse P3: Innovative cyclophotocoagulation. Rom J Ophthalmol. 2017;61(2):107-111.

