







Until recently, our approach as glaucoma physicians has been reactive when strategizing care for our patients. We would wait for the disease to progress before incrementally advancing therapy. Then, we repeat the process, while hoping that our patient would retain good functional vision before having their glaucoma progress to an end stage.
This philosophy, unfortunately, doesn’t work well for us and those we care for. In the best-case scenario, the glaucoma would be controlled just enough to prevent progression; however, any slip-up would result in further damage. Given that adherence rates to medical therapy are poor, the ideal situation of keeping the glaucoma at bay simply couldn’t be achieved with enough consistency. The result was that our patients lost vision and at times even went blind. For those of you who are football fans, this is equivalent to your team going into a “prevent defense” at the end of the game. If you are unfamiliar with this analogy, this means that the defensive strategy your team uses is to play as safe as possible to avoid losing — they would react only when needed. The usual outcome to this approach was that the team would either barely win or quite frequently lose. Either result is nerve wracking to watch.
The question many of you probably have is why anyone would ever take such a reactive approach if it yields such bad outcomes, whether it be in a sporting event or in glaucoma care. The answer in the case of glaucoma is that this was the best plan we had based on the options that were available. Our team was limited in talent, so it was the only philosophy we could apply even if that meant patients were losing vision. This is based on limitations in 2 key areas: diagnosis and treatment.
Overcoming Barriers in Glaucoma Care
The trouble with glaucoma diagnostics was that all modalities required a loss of retinal ganglion cells (RGCs) and optic nerve tissue. Despite the introduction of OCT that permitted the identification of structure before functional loss (which was a big deal), it still required the death of nerve tissue. In an ideal setting, we would want to locate stressed but not yet atrophied RGCs, and then we help them survive through the reduction of timely and effective IOP reduction. But this capability didn’t exist.
Another cause that led to this reactive strategy is that even if we could identify these distressed cells, our treatment paradigm didn’t have a very effective and reliable solution. This is because we depended on topical eye drops. We know that nonadherence rates to glaucoma medical therapy are high. It is no wonder that our approach had to be reactive in nature — we simply didn’t have the tools, or players, to implement another game plan.
Fortunately for us and our patients, we have new options. Our glaucoma team has drafted 2 stars: electroretinography (ERG) and selective laser trabeculoplasty (SLT). ERG improves our diagnostic capabilities and SLT strengthens our timeliness for therapeutic options. The addition of these allow us to take a proactive, instead of reactive, approach by filling 2 critical gaps. Electroretinography enables the identification of stressed RGCs before irreversible structural changes occur, while SLT provides IOP reduction that eliminates the issue of patient nonadherence to eye drops.1,2
Electroretinography
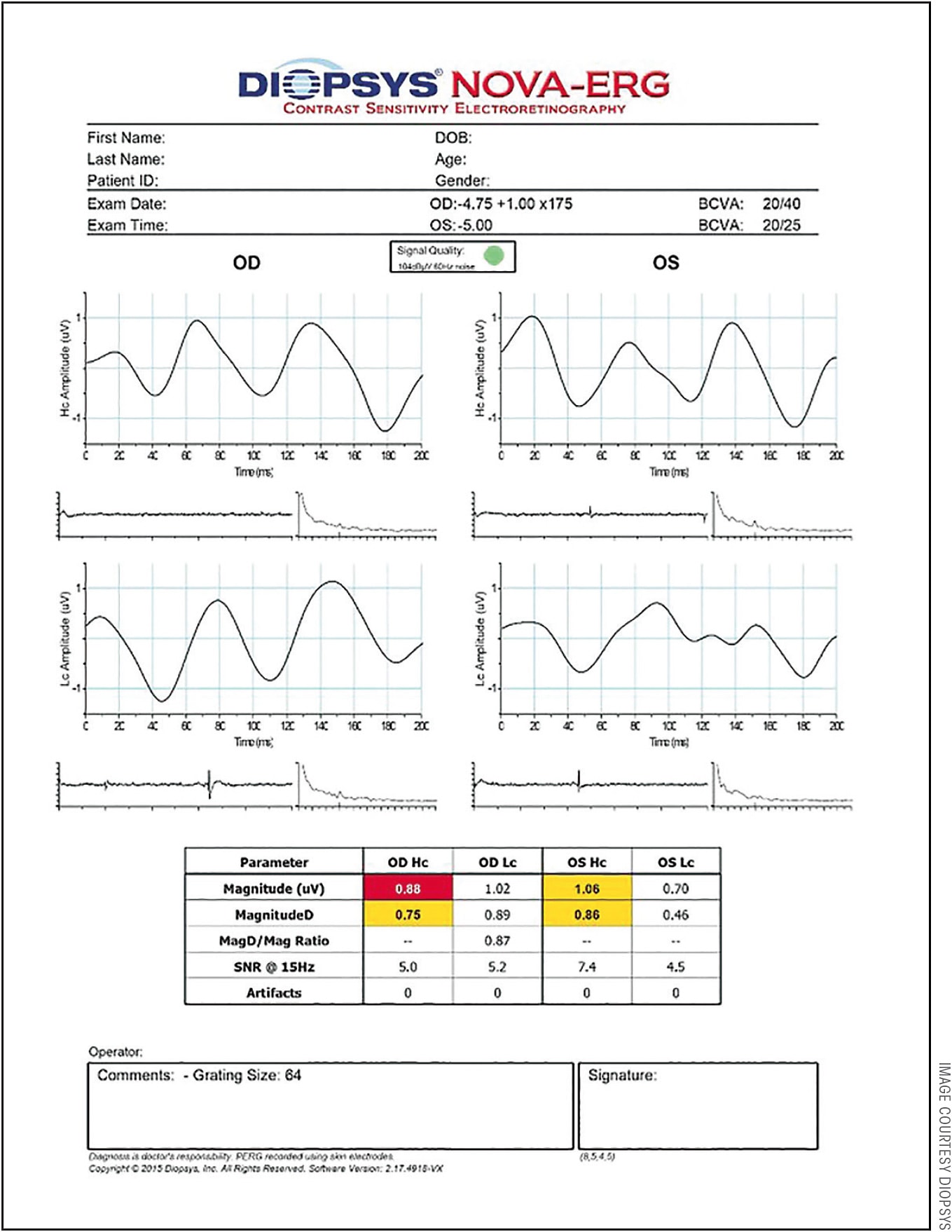
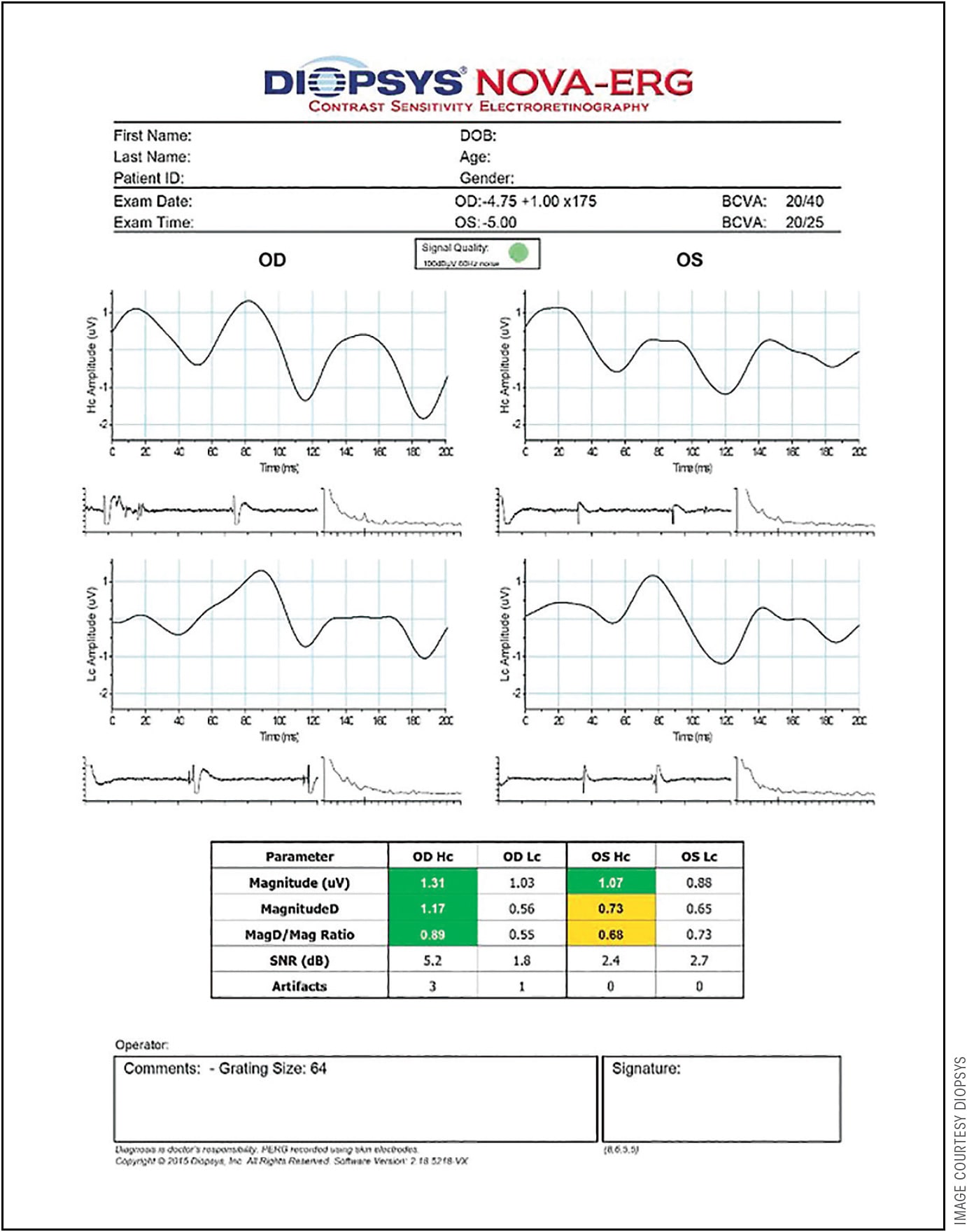
Let’s take a closer look at the new players, beginning with ERG. When the root cause of glaucoma is broken down, the key anatomical change is at the level of RGCs. The loss of these cells and their output is what eventually breaks the neuronal pathway from the eye to the brain. This then leads to the following question that needs to be answered for every patient: is the current pressure too high, that without a reduction in IOP, these conditions will lead the susceptible RGCs to atrophy? Through the application of ERG, especially the use of certain applications like pattern electroretinography (PERG) that isolate the function of the ganglion cells in the inner retina, the decrease in the ability to produce action potentials from these cells due to stress can be practically identified. More importantly, it has been shown that with adequate and timely IOP reduction, the at-risk RGCs can return to normal functioning — they have not crossed the critical point of no return (Figures 1 and 2).3 They can be saved without permanent damage.
This all might sound great, but you might be saying, this technology is not new, so why haven’t we used it before? The major hurdle to the commonplace use of ERG was the complexity of the technology that was older and existed in large hospitals and institutions. These antiquated machines were not available in a typical outpatient setting where most eye care providers practice. The machinery was bulky, which required an undesirably large footprint. It was also very expensive not only to own but also to operate, because it necessitated skillful technicians. To complicate these matters, the test itself was long and uncomfortable for patients. Once the measurements were obtained, the time and expertise needed to analyze the data were significant. It is no wonder that ERG was not commonly used.
But with time, technology improves, as has ERG. Several manufacturers addressed these critical shortcomings and enabled the availability of ERG to the average practitioner in an office environment. Upgrades to computer-based technology, disease-specific algorithms, and testing applications improved the physician’s capability to measure dysfunction in the retina at the root of disease development. These tests are available and used for the same purposes as those in the institutional setting.
The Diopsys system is small and portable, requiring less space and expenditure. The ancillary support needed to run the test is comparable to training a technician about automated visual field testing and having them run it. Usually it can be performed in 25 minutes or less with printouts that are easy enough to understand and appear very similar to OCT testing. The learning curve is fast.
Selective Laser Trabeculoplasty
Now with ERG helping on the defensive diagnostic side, we can shift our attention over to our offensive player, SLT. Although the exact mechanisms are not understood, the use of SLT is known to be an effective method of IOP reduction. Its use as first-line therapy can result in IOP decreases of approximately 25% to 30% from baseline measurements. Just like with any other therapy, an assessment of risks needs to be accounted for a proper understanding. These are generally low and infrequent but can include post-laser IOP spikes. However, the summation of these risks from SLT are generally still far less than the amount of damage caused by the standard nonadherence of patients with eye drop therapy.
Again you might be asking, just like ERG, don’t we already have this? Selective laser trabeculoplasty has been around for years, but our current utilization of this technology is low, especially in the United States. It may come as a surprise to some providers, but SLT is used much more frequently in other countries. This includes early treatment to initiate IOP-lowering therapy even before the use of any eye drops all the way through to even after glaucoma surgery is performed. However, in the United States, the uptake of SLT is limited.
Interestingly, there is an apparent disconnect. Let me illustrate with an example that I have seen countless time. In a clinical medical education setting that utilizes audience response, the question is posed as to what modality to utilize when initiating IOP-lowering therapy in a newly diagnosed patient. Choices include eye drops, laser, and surgery. The most common answer is an eye drop, beginning with a prostaglandin analogue. When the question is changed subtly to what modality would you, as the doctor, want for yourself, most respond SLT. Why is there a difference in how the physician would treat an average patient as opposed to him- or herself? The fact is that physicians have a clearer and deeper understanding to the benefits and risks of SLT compared to eye drop therapy. Most doctors would elect to assume the small relative risks of SLT therapy over the more common side effects (hyperemia in particular) and need for compliance with everyday topical applications.
Some argue the disconnect stems from the doctor’s limited time to explain SLT and/or the perception from patients about having a laser procedure instead of using drops. However, if most doctors would have SLT before eye drop therapy, shouldn’t this translate to our patients? Also, with the rapid uptake of MIGS along with the associated change of considering glaucoma an interventional instead of a medically managed disease, the utilization of SLT should come sooner and more frequently in the treatment paradigm. Why stop this evolution of care and accept a secondary “MIGS and meds” result, which is common to see, when there can be a “MIGS and SLT” solution?
ETHNICITY AND GLAUCOMA By Mark A. Latina, MD
Glaucoma is a leading cause of blindness among African Americans. At least 8% will develop glaucoma in their lifetime. More importantly is glaucoma’s effect on vision in this population. The Salisbury Eye Evaluation Study revealed that blacks are 15 times more likely to be visually impaired from glaucoma than whites.1 In addition to glaucoma being more prevalent in individuals of African descent, glaucoma may cause a disproportionally higher rate of functional impairment compared to those of European descent. Studies suggest that glaucoma tends to occur at an earlier age and these individuals present with more extensive damage at diagnosis.2 Also, studies suggest that the disease may progress at a faster rate in individuals of African descent and they may have lower levels of adherence to treatment, thereby making them more vulnerable to progressive visual field loss and vision loss from glaucoma which is due to progressive loss of retinal ganglion cells.3
Because glaucoma in African Americans may be more aggressive, early detection and early treatment, in particular, is critical to preventing blindness in this population. Bode et al showed that in glaucoma suspects, pattern electroretinography (PERG) changes can occur up to 8 years before structural OCT changes in the retinal nerve fiber layer.4 Therefore, an abnormal PERG in this population would be an important test to alert the physician to follow a patient closely and/or to consider instituting therapy.
Delayed diagnosis can impact a patient’s quality of life. Furthermore, late detection of glaucoma results in a four-fold increase in the costs of treating this disease. The key is early detection, and electrophysiology combined with selective laser trabeculoplasty can play an important role in this.
Dr. Latina is an associate clinical professor at the New England Medical Center, Tufts University School of Medicine.
Dr. Latina invented selective laser trabeculoplasty. He reports consultancy to Diopsys.
References
- Freeman EE, Muñoz B, West SK, Jampel HD, Friedman DS. Glaucoma and quality of life: the Salisbury Eye Evaluation. Ophthalmology. 2008 Feb;115(2):233-238.
- Martin MJ, Sommer A, Gold EB, Diamond EL. Race and primary open angle glaucoma. Am J Ophthal. 1985;99(4):383-387.
- Greenidge KC, Dweck M. Glaucoma in the black population: a problem with blindness. J Natl Med Assoc. 1988;80(12):1305-1309.
- Bode SF, Jehle T, Bach M. Pattern electroretinogram in glaucoma suspects: new findings from a longitudinal study. Invest Ophthalmol Vis Sci. 2011;52(7):4300-4306.
ERG, SLT, AND GLAUCOMA’S ECONOMIC BURDEN By Thomas K. Mundorf, MD
The economic burden of glaucoma is seeing extreme growth, due in large part to population growth, especially aging baby boomers. The glaucoma therapeutics market is projected to rise 33% (from $5.6 billion to $7.6 billion by 2024).1 In January of 2018, Valeant Pharmaceuticals noted the market for glaucoma was going to increase from $6 billion to $11 billion by 2020 (an 83% increase).2
The financial burden of glaucoma increases as disease severity increase. A study by Varma et al found a 4-fold increase in direct ophthalmology-related costs as severity increased from asymptomatic ocular hypertension/earliest glaucoma (stage 0) through advanced glaucoma (stage 3) to end-stage glaucoma/blindness.3
The diagnosis of glaucoma requires optic nerve damage. Direct observation of the optic nerve gives us an impression of its health. Ocular coherence tomography (OCT) provides data to compare our patients to a normal data base. Visual fields document loss of performance. Both OCT and perimetry verify past damage. Limiting damage is the goal of the eye physician and finding it as early as possible is mandatory. Having the technology that could predict injury before permanent damage occurs is almost priceless. Electrophysiology appears to be the practical technology that we can add to our practice to meet this need.
Ophthalmologists agree that patient compliance is one of our biggest hurdles. The cost of medicines, brand or generic, is a major factor in adherence. Dosing and side effects (topical and systemic) further contribute to patients not implementing their doctor’s instructions. This results in lack of control of their glaucoma, which then leads to further damage, loss of function, and overall diminished quality of life and burden to health care. Laser trabeculoplasty, in the past relegated to second- or third-line therapy, is now moving to the forefront. Selective laser trabeculoplasty (SLT) is well tolerated, repeatable, economical, and well accepted by patients earlier in the course of their treatments. This can offer improved control of intraocular pressure (IOP), a better prognosis, and reduced health care costs.
References
- Glaucoma Therapeutics Market: Snapshot. SB Wire. April 11, 2017. Available at http://www.sbwire.com/press-releases/glaucoma-therapeutics-market/release-792628.htm .
- Welsh T. Valeant: what does papa’s new promise mean for the company? January 10, 2018. Available at https://seekingalpha.com/article/4136708-valeant-papas-new-promise-mean-company .
- Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011 Oct; 152(4):515-522.
Dr. Mundorf is founder of Mundorf Eye Center in Charlotte, North Carolina. He reports no related disclosures. Reach him at tommundorf@aol.com.
Incorporating New Technology
There is really just one hurdle left that must be addressed beyond the addition of ERG and SLT, and this is the biggest but also the most hidden of them all. The glaucoma physician, who is the coach of the team, must recognize these players and incorporate them by applying a proactive strategy.
Without this philosophical shift in our therapy paradigm, we will never be able to take on this new approach. We should change our old thought process of letting glaucoma progress and responding in only a bare minimum way. Instead, we can take advantage of what is now available and intervene before loss even occurs. In other words, let’s play to win the game as opposed to hoping we just don’t lose. GP
References
- Banitt, MR, Ventura LM, Feuer WJ, et al. Progressive loss of retinal ganglion cell function precedes structural loss by several years in glaucoma. Invest Ophthalmol Vis Sci. 2013;54(3):2346-2352.
- Mavilio A, Scrimieri F, and Errico D. Can variability of pattern ERG signal help to detect retinal ganglion cells dysfunction in glaucomatous eyes? Biomed Res Int. 2015;2015:571314.
- Ventura, LM, Feuer WJ, and Porciatti V. Progressive loss of retinal ganglion cell function in hindered with IOP-lowering treatment in early glaucoma. Invest Ophthalmol Vis Sci. 2012;53(2):659-663.
