







For the last several decades, various authors have described the success of trabeculotomy in treating different types of open-angle glaucoma (OAG).1-5 Trabeculotomy lowers IOP by enhancing the flow of aqueous through the inherent blocked drainage system of the eye (Schlemm’s canal and the adjacent collector channels). Most notably, this surgery does not create a bleb, a significant long-term safety factor, on the surface of the eye.
We recently reported a novel, minimally invasive approach to a circumferential ab interno trabeculotomy: gonioscopy-assisted transluminal trabeculotomy (GATT)6-8 in congenital and juvenile glaucoma, adults with various OAGs and in eyes with prior incisional glaucoma surgery.
In this article, we will briefly discuss the results of GATT, key surgical pearls to optimize outcomes and strategy to optimize postoperative care. We will end with a brief discussion of ab interno canaloplasty (ABiC) and areas of future concern.
We have previously published on the key surgical steps of GATT and so will not reference them here (for more information and videos, visit www.glaucomaassociates.com ).6-9
GATT results
The short- and long-term outcomes of GATT demonstrate that this technique is an effective method for treating various forms of OAG. In our primary open-angle glaucoma group, the average IOP decreased by 9.2 mm Hg from baseline with a decrease in 1.43 anti-glaucoma medications at 24 months. The mean percentage of IOP decline in this group was 37.3%. In patients with secondary open-angle glaucoma, the average IOP decreased by 14.1 mm Hg on 2.0 fewer medications at 24 months. The mean percentage of IOP decline in this group was 49.8%.10
Additionally, we reported on outcomes of GATT in our primary congenital glaucoma group and juvenile open-angle glaucoma group. In this study, 14 eyes of 10 patients underwent GATT with greater than 12 months follow-up. The mean IOP decreased from a baseline of 27.3 mm Hg to 14.8 mm Hg and the mean number of antiglaucoma medications decreased from a baseline of 2.6 to 0.86 at 12 months.7
We have also successfully used GATT to surgically manage patients who have previously failed a traditional incisional glaucoma surgery, such as a trabeculectomy or a glaucoma drainage implant.8 In this patient population, we treated 35 eyes of 35 patients who previously underwent an incisional glaucoma surgery. At baseline, the mean IOP was 25.7 mm Hg on 3.2 antiglaucoma medications. At 24 months, the mean IOP decreased to 15.4 mm Hg on 2.0 medications. This study demonstrated that a GATT surgery could be successful in patients who previously underwent surgeries in which aqueous was shunted away from the normal collector pathways. In the vast majority of these patients, we re-established aqueous flow through their trabecular outflow system using an ab interno, conjunctival-sparing approach.
What’s old is new again
One exciting aspect of GATT is that it modifies an established surgery performed since the 1960s.1-5,11 When compared to the historic results of ab externo trabeculotomy, GATT has similar if not better outcomes. For example, Tanito et al reported an IOP of 16.1 mm Hg on 0.7 glaucoma medications at one year in patients who underwent trabeculotomy when combined with cataract surgery.12 More recently, Chin et al reported on a modified circumferential ab externo trabeculotomy with a mean postoperative IOP of 13.1 mm Hg on a mean number of 0.5 glaucoma medications at one year.13 We feel the minimally invasive aspect of GATT is promising, given the absence of conjunctival and scleral incisions and scarring, which may contribute to failure of future filtration surgery.
Improving success rates
In order to improve outcomes and maximize success following GATT, we have developed certain modifications and strategies during surgery as well as throughout the postoperative period. The vast majority of patients have a hyphema after the GATT surgery. This is likely related to an intact collector system that allows blood to reflux into the eye immediately after surgery when the IOP is relatively low. To protect against immediate postoperative hypotony and hyphema, we leave a 15% to 50% Healon fill in the anterior chamber, depending on the degree of blood reflux seen during surgery and the extent of the episcleral venous fluid wave seen intraoperatively.14 Another strategy that helps minimize the hyphema risk is to avoid GATT in patients who cannot be taken off all anticoagulation medication.
Other relative contraindications for GATT include an unstable IOL, poorly visualized or appreciated angle anatomy, extensive peripheral anterior synechiae, or severe Fuch’s dystrophy (or endothelial compromise). Also, certain relative contraindications for GATT include eyes with a difficult angle view due to corneal pathology, a prior corneal transplant or an inability to properly identify key angle anatomy.
Keeping one’s head elevated at 30° for two weeks following surgery also allows for rapid resolution of the hyphema. If patients cannot elevate their head for at least the first 14 postoperative days, we reconsider performing a GATT. During the surgery, we also have the patient in a reverse Trendelenburg position, which allows for optimal visualization of the angle during surgery by minimizing the risk of blood reflux into the eye.
Benefits of a suture
Surgeons can safely perform GATT with a microcatheter (250A iTrack Microcatheter, Ellex) or a suture with a cautery-blunted tip (we prefer 5-0 Prolene or 5-0 nylon if Prolene is not available).9 Performing this surgery with a suture that costs $5-$10 has tremendous implications for cost-effective health-care delivery in both developing and developed nations (the microcatheter costs $750 to $1,000).
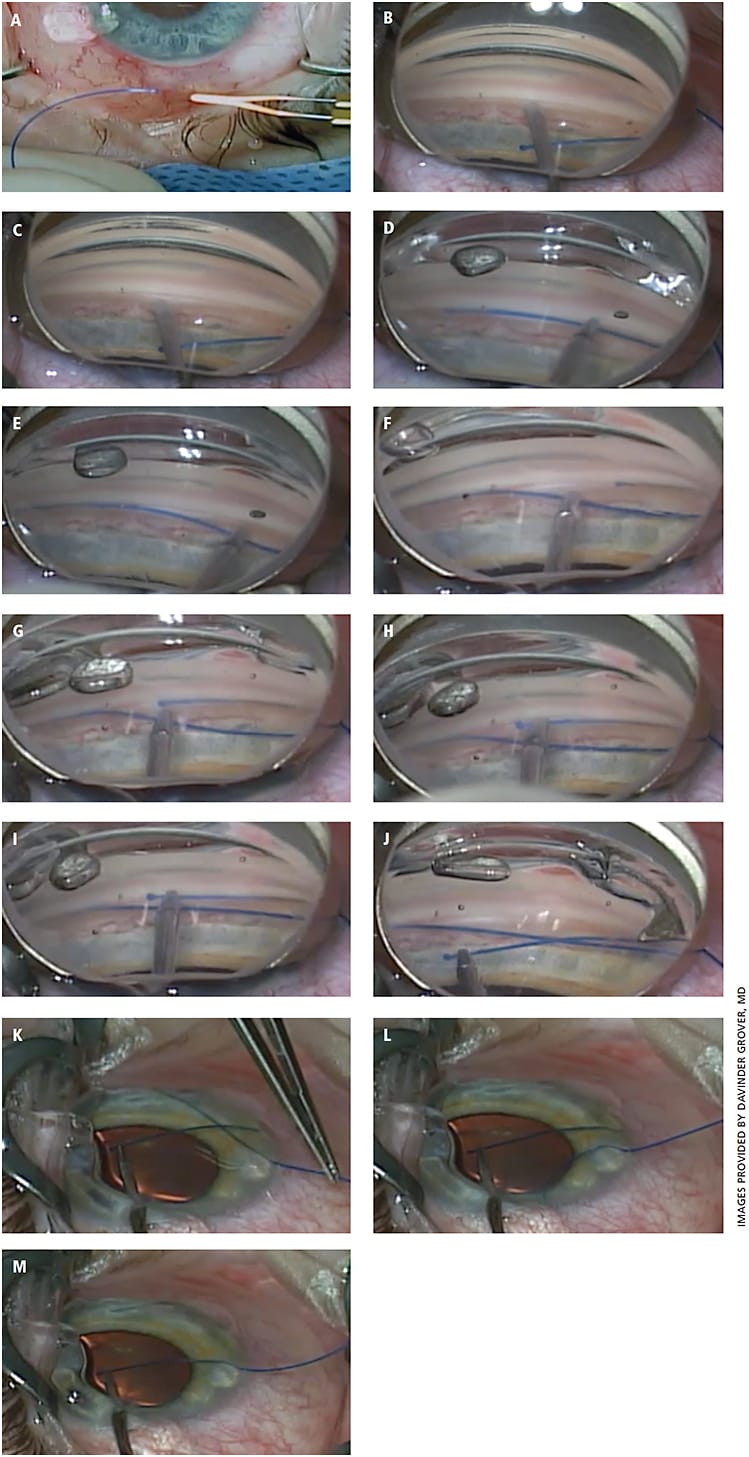
While it is easier to learn the basics of the technique using the microcatheter, surgery can be performed just as easily using a 5-0 Prolene suture, once one is comfortable with this technique (Figure 1). We have not found any outcome differences between GATT surgeries performed with a suture or with a microcatheter.
ABiC
Some surgeons are performing ab interno canaloplasty (ABiC), a modified GATT technique.15 Even though an ab interno trabeculotomy is not performed, viscodilation is, at 360°. Also, unlike classic canaloplasty, a retention suture is not left behind.
Some surgeons say that this technique provides successful outcomes; however, to date, no peer-reviewed literature has reported short- or long-term outcomes on this approach. We eagerly await long-term, peer-reviewed, published results on this novel technique but, at this time, prefer to cleave open the canal as in classic trabeculotomy, which has a longer historical track record.

Conclusion
Canal-based procedures continue to evolve in a very favorable manner, providing us better ways to care for our patients. However, we still lack information regarding wound healing, which could adversely alter the outcome of angle surgery in some patients.
Modulation of wound healing in the canal is in its infancy; it took us more than 50 years to improve wound healing for filtration procedures. We are optimistic that we will learn to modulate in-the-angle wound healing in a much shorter period of time. In addition, we need an “aqueous outflow map,” a technology to quantify flow in the canal system, to better understand why these procedures work and why they fail.
We are in a new renaissance era for angle-based glaucoma surgery. We, along with many of our colleagues, look on with excitement for continued innovation in MIGS as well as improved glaucoma surgical care for our patients. OM
REFERENCES
- Harms H, Dannheim R. Epicritical consideration of 300 cases of trabeculotomy ‘ab externo.’ Trans Ophthalmol Soc UK. 1970;89:491-499.
- Gregersen E, Kessing SV. Congenital glaucoma before and after the introduction of microsurgery: results of ‘macrosurgery’ 1943-1963 and of microsurgery (trabeculotomy/ectomy) 1970-1974. Acta Ophthalmol (Copenhn). 1977;55:422-430.
- Haas J. Principles and problems of therapy in congenital glaucoma. Invest Ophthalmol. 1968;7:140-146.
- Smith R. A new technique for opening the canal of Schlemm: Preliminary report. Br J Ophthalmol. 1960;44:370-373.
- McPherson SD Jr, McFarland D. External trabeculotomy for developmental glaucoma. Ophthalmology. 1980;87:302-305.
- Grover DS, Godfrey DG, Smith O, et al. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014;121:855-861.
- Grover DS, Smith O, Fellman RL, et al. Gonioscopy assisted transluminal trabeculotomy: an ab interno circumferential trabeculotomy for the treatment of primary congenital glaucoma and juvenile open angle glaucoma. Br J Ophthalmol. 2015;99:1092-1096.
- Grover DS, Godfrey DG, Smith O, et al. Outcomes of Gonioscopy-assisted Transluminal Trabeculotomy (GATT) in Eyes With Prior Incisional Glaucoma Surgery. J Glaucoma. 2017;26:41-45.
- Grover DS, Fellman RL. Gonioscopy-assisted Transluminal Trabeculotomy (GATT): Thermal Suture Modification With a Dye-stained Rounded Tip. J Glaucoma. 2016;25:501-504.
- Grover DS. Gonioscopy-Assisted transluminal trabeculotomy (The GATT procedure): An ab interno circumferential trabeculotomy – Mid-term follow up. Paper presented: American Academy of Ophthalmology Annual Meeting 2015; November 17, 2015; Las Vegas.
- Smith R. Nylon filament trabeculotomy. Comparison with the results of conventional drainage operations in glaucoma simplex. Trans Ophthalmol Soc N Z. 1969;21:15-26.
- Tanito M, Ohira A, Chihara E. Surgical outcome of combined trabeculotomy and cataract surgery. J Glaucoma. 2001;10:302-308.
- Chin S, Nitta T, Shinmei Y, et al. Reduction of intraocular pressure using a modified 360-degree suture trabeculotomy technique in primary and secondary open-angle glaucoma: a pilot study. J Glaucoma. 2012;21:401-407.
- Fellman RL, Grover DS. Episcleral venous fluid wave: intraoperative evidence for patency of the conventional outflow system. J Glaucoma. 2014;23:347-350.
- Khaimi MA. Canaloplasty: A Minimally Invasive and Maximally Effective Glaucoma Treatment. J Ophthalmol. 2015;2015:485065.
About the Authors

