







Learning from ‘the worst of the worst’
Cataracts, that is. Johnny Gayton has discerned much from his patients. He shares those thoughts worldwide.
By Christine Bahls, Executive Editor
Johnny Gayton, MD, likes to think outside the squared parallelogram. If those thoughts are worth it, he acts on them.
It’s a process that has served him, his ophthalmic brethren and his community for over 30 years. During that time, through observation and deduction, he developed a more efficient surgical technique to remove cataracts, a way to save the sight of narrow-angle glaucoma patients and how to insert two intraocular lenses (IOLs) in the same eye.
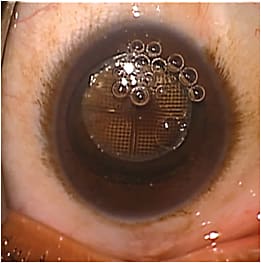
View of a hypermature lens that is becoming black, which can take a while to remove for they are hard to break up
The processes, the temporal approach to cataract surgery, lens removal to open anatomically narrow angles, and the so-called piggyback, are now considered standard operating procedures.
All the right ingredients
When Dr. Gayton began his practice in Warner Robins, Ga., it was primarily rural territory. (It is rural no longer: In 2012, CNN Money named it the 7th best small U.S. city to live in.)
Its citizenry, and those who lived near and far, did virtually everything right to grow the worst cataracts possible.
Then, illiteracy wasn’t rare. Smoking and eating the wrong foods were problems. Unfortunately fear has been a serious factor: Many patients face blindness before coming to Dr. Gayton, their anxiety over facing surgery that great. He has seen his share, and then some, of black cataracts.
“I frequently deal with the worst of the worst,” says Dr. Gayton, the man who gets the referrals. These referrals also include many end-stage glaucoma patients; one waited until her IOP was 78 mm Hg before coming in, he says.
The challenge of it all
Dr. Gayton says he loves what he does because he can help bring sight back to the unsighted. Warner Robins, through Dr. Gayton’s social media testimonials, knows it. It’s the challenge of it all.
Some of these hypermature cataracts take 45 minutes or longer to remove, as compared to the standard five to eight minutes. “Two days before Thanksgiving I started working on what I thought was a white cataract and found a dense red nucleus under the milky white cortex. It was very difficult to remove. The cataract was in a retired, elderly lady. She lived alone but could still get around in familiar settings. Unfortunately, no one was paying attention to the fact that she was holding on to the furniture to find her way. She had a very dense brown cataract in one eye and that red/white combination in the other.”
Thanksgiving, says Dr. Gayton, “was the first day that she had seen well in years.”
Red, white, dense brown, and even black cataracts are commonly faced in his practice. Over the past two years he has removed many of the red and black cataracts with femtosecond laser assistance in order to decrease the energy required.
While any femto will generally handle the capsule, his practice needs a laser that will effectively treat very hard nuclei. He has chosen one that has a liquid optics interface to handle these hypermature cataracts.
“I have talked with other people who have used other lasers and most agree: a liquid optics interface allows the laser to perform nuclear fragmentation more effectively.”
Observation, deduction and response
Dr. Gayton, a Georgia native, hadn’t intended to be primarily a cataract and glaucoma surgeon (and a high-volume one at that). He planned to be a general ophthalmologist, primarily providing care for his local community. But in those early years of his practice, fate, his thought-and-deduction process and the unique characteristics of middle Georgia intervened.
In the early 1980s, he noticed a preponderance of narrow angle glaucoma patients, some of whom had lost their sight following angle closure even after a peripheral iridectomy. Two developments arose: he began removing the lenses of many glaucoma patients with a narrow angle, convinced that such surgery would prevent angle closure.1 And, because so many narrow-angle patients are nanophthalmic with severe hyperopia, he devised the piggyback procedure for inserting IOLs.2
The following, written by Dr. Gayton, appeared in David F. Chang’s book, Curbside Consultation in Cataract Surgery: 49 Clinical Questions:3
“Anatomically, narrow angles are a worldwide problem, but they are especially common in rural Georgia. Many of the eyes with narrow angles are hyperopic. This high incidence of hyperopia led me to develop the piggyback lens technique in an effort to better rehabilitate these eyes following lens surgery.
…. I explain [the increasing narrowing] to the patient by describing that the lens grows in circumference by adding rings like a tree …. Many patients with narrow angles will ultimately develop angle closure …. After witnessing several cases of blindness, even in patients who had laser iridotomies, I concluded that the best treatment for narrow angles is lens removal.
Dr. Gayton then went on to describe the piggyback.
About this same time he also devised the temporal approach for cataract surgery. The reason? His concern was that many postoperative cataract patients developed a lot of against-the-rule astigmatism over time. He found that by moving to the side this against-the-rule drift was virtually nonexistent. As he told this publication a few years ago, “As we’ve made our incisions smaller, there’s much less influence on astigmatism.”4 But he still strongly believes that cataract surgery is safer, easier and more predictable when performed from a temporal approach.
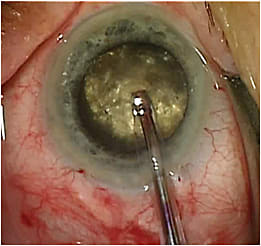
Close-up of a black cataract.
Preaching what he practices
For many years, Dr. Gayton has been a strong proponent of educating the local community about eye care. He does this by serving on the faculty of the local medical school, appearing on television and radio and giving newspaper interviews. “I am training as many primary care physicians as I can to recognize eye problems …. I also go on newscasts and talk shows. It’s definitely been a challenge to get people to understand the need for early diagnosis and treatment.”
Dr. Gayton hasn’t confined his education efforts to his local community. “I launched the toric IOL in my home state and in the nations of China and Hungary and launched phacoemulsification in Mongolia. I would imagine that I have given around 1,000 lectures worldwide.”
Since there are still people in his community — and everywhere else — who have poor diets, smoke and don’t protect their eyes from the sun and visual demands are increasing, his practice is seeing more and more cataracts in young adults.
“So the education is working,” says the man who has performed at least 55,000 cataract surgeries over his career. “But there are still people who fall through the cracks. Some people, despite your efforts, are not going to get it, and they are going to wait too long.” OM
Dr. Gayton’s financial disclosures:
• Bausch & Lomb/Valeant: Consultant
• Abbott Medical Optics/OptiMedica: Consultant
• Omeros: Consultant
REFERENCES
1. Gayton JL, Van der Karr MA, Sanders V. Combined cataract and glaucoma procedures using temporal cataract surgery. J Cataract Refract Surg. 1996; 22:1485-1491.
2. Gayton J, Sanders V, Van Der Karr M et al. Piggybacking Intraocular Implants to Correct Pseudophakic Refractive Errors. Ophthalmol. 1999;106:56-59.
3. D F Chang, Ed. Curbside Consultation in Cataract Surgery: 49 Clinical Questions. Slack, Inc. Jan. 1, 2007. P. 81.
4. Are you on a plane with the best? Ophthalmology Management. April 1, 2003. . Accessed May 8, 2015.