







My Go-To IOL for Patients with Previous Corneal Refractive Surgery
The nanoFLEX® Collamer® lens provides excellent depth of field and also enables a solution for refractive surprises.
By Robert W. Snyder, MD, PhD
As every cataract surgeon knows, the majority of patients who’ve had corneal refractive procedures such as RK, LASIK or PRK don’t know their preoperative refractive status or the treatment parameters that were used. Although some new IOL power calculation formulas have been designed specifically for use in this group of patients, it’s still difficult to calculate their IOL power as precisely as we’d like. As a result, we see post-op “refractive surprises” more frequently among these patients than among those who haven’t undergone corneal refractive surgery. We face this challenge more and more as time goes on because PRK and LASIK, both popular procedures, have been available for more than 20 years.
For my cataract surgery patients who previously had corneal refractive surgery, I have a go-to intraocular lens, the nanoFLEX® Collamer® IOL. This is my preferred IOL for these patients for two reasons. First, patients are very happy with the quality of their vision after cataract surgery. The aspheric design and physical characteristics of the lens provide excellent depth of field. A significant percentage of my patients with a nanoFLEX IOL targeted for distance see 20/20 at distance and J3 at near, which is uncommon with other monofocal lenses.
A Solution for the Refractive Surprise
The second reason the nanoFLEX is the IOL I prefer for cataract surgery patients who have previously had corneal refractive surgery is that I can use the WaveScan WaveFront System (Abbott Medical Optics) to obtain a useful wavefront measurement with this lens in the eye. I can then perform a wavefront-guided surface ablation to correct residual refractive error, i.e., “refractive surprises.” (Note that this is an off-label procedure.) The ability to obtain a usable WaveScan through a nanoFLEX lens relates to the optical properties of the Collamer material. The hydrophilic nature of Collamer gives the IOL an ultra-high water content (40%) and a relatively low index of refraction. Thus, to achieve the desired IOL power the curvature is steeper than that of most other IOLs (Figure 1). Therefore, the amount of light reflected off the front surface is much less than with other IOLs (Figure 2). Obtaining a usable WaveScan through acrylic IOLs isn’t possible because the reflected light creates a large “blob” of reflected light in the center of the scan that prevents the system from calculating a treatment.
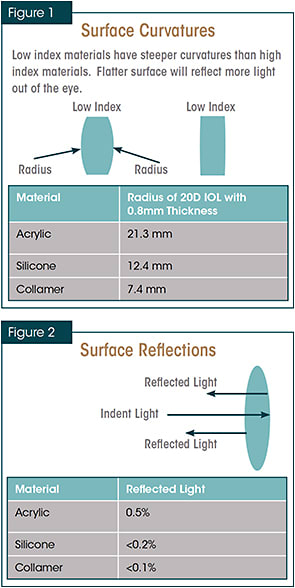
Figures 1 and 2. Diagrams courtesy of Jim Schwiegerling, PhD.
In 2013 at ASCRS, my colleagues and I presented a poster, showing a small series of cases using the WaveScan and off-label wavefront-guided PRK to fix refractive surprises after cataract surgery in patients who previously had corneal refractive surgery.1 This series included cases in which the original corneal refractive procedure created a decentered optical zone or irregular astigmatism. We’ve been quite pleased with our outcomes (Figures 3 and 4) and the ability the nanoFLEX lens gives us to help this group of patients achieve the best possible vision.
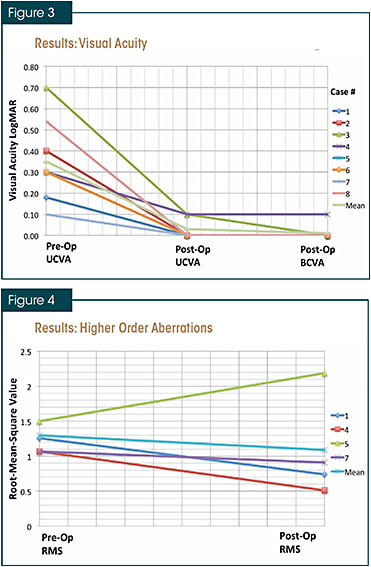
Figures 3 and 4. In eight eyes of five patients who underwent off-label wavefront-guided PRK with iris registration to correct residual refractive error following cataract surgery, UCVA improved, BCVA improved or remained the same, and mean higher-order aberrations measured by RMS error decreased. All of the patients had corneal refractive surgery at some point prior to cataract surgery.
A Few Caveats
Post-refractive surgery patients may be used to excellent uncorrected vision and their expectations are high. These patients require some extra education right from the start so they understand that even with a perfect surgery and state-of-the-art IOL calculations, their IOL power could be off by three-quarters of a diopter or more, perhaps necessitating an additional procedure. I let them know we have a possible solution for this residual post-cataract refractive error. However, it’s also important to perform an appropriate consent and clearly explain that this is off-label, not approved by the FDA and hasn’t undergone rigorous peer-reviewed testing.
I don’t recommend the nanoFLEX IOL for patients who have pseudoexfoliation syndrome. The lens fills the capsular bag, which may result in some tension on the bag. With pseudoexfoliation, I’m already concerned about zonular laxity and anterior capsular fibrosis, so I prefer to avoid the possibility of stimulating either any further. I also avoid using this IOL in patients with a history of trauma. If a maneuver has to be performed to re-position the lens, it’s easier to perform if the lens has a C-loop haptic style rather than a plate configuration.
The Surgical Steps
In the OR, the nanoFLEX lens is technically simple for the technicians to load into the injector and easy for me to inject into the eye and push into the bag with the nucleus rotator. I create a 6 mm to 7 mm capsulotomy, which usually collapses to less than 6 mm. I’m fastidious about cleaning the cortex and polishing any cellular clumps or debris from the posterior capsule. I also polish the undersurface of the anterior capsule after the lens has been delivered and before the viscoelastic is removed. I believe this helps to prevent fibrosis, capsular contraction and potential posterior shift of the bag /IOL that I’ve observed on rare occasion.
In summary, I choose the nanoFLEX Collamer IOL for my post-refractive-surgery cataract patients because it gives them a high quality of vision and often extended depth of field and thus gives me an opportunity to meet the high expectations of these individuals who have experienced the benefits of refractive surgery. The nanoFLEX also allows a strategy for fine-tuning their results when it is necessary. ■
Reference
1. Imbornoni LM, Hunter BA, Schwiegerling J, Snyder RW. Wavefront-guided PRK for refractive error following cataract extraction with aspheric IOL implantation. Poster presentation at the annual meeting of the American Society of Cataract and Refractive Surgery, April 2013, San Francisco, CA.

| Dr. Snyder is a cataract and refractive surgeon serving patients in Tucson, Green Valley and surrounding areas of southern Arizona. He is also a Professor of Biomedical Engineering at the University of Arizona. |