







Manage MGD to stem dry eye
New diagnostic tools, treatments make doing both easier.
By Kendall E. Donaldson, MD, MS and Kendra Davis, COA

The meibomian glands may not be the feature of the eye that originally attracted any doctor to choose ophthalmology as a profession, but treating meibomian gland dysfunction (MGD) has developed its own intrigue and appeal over the last few years.
LOOKING UNDER THE LIDS
The missing link
The turning point in treatment of ocular surface disease occurred when Michael Lemp subcategorized dry eye (see Table 1), determining that the lids were the missing link behind evaporative dry eye disease.1 As a crucial component of the ocular surface and the primary inciting factor in the bulk of our dry eye patients, it is necessary to manage MGD to achieve optimal treatment in dry eye patients.
| SUBTYPE OF DRY EYE | CHARACTERIZATION |
|---|---|
| 86% - Evaporative-lipid deficient caused by MGD | Occurs when the water (or aqueous) in tears evaporates at a faster rate than normal |
| 14% - Aqueous deficient | Occurs when aqueous generation from the lacrimal gland is insufficient to keep the eyes moist |
Industry investment
A second turning point occurred when industry began investing in ocular surface disease and the development of non-covered diagnostic and treatment options. To ophthalmologists, dry eye was an enigma; subjective diagnosis and assessment, a dilemma; and treatment, a conundrum. Early attempts at treatment resulted in nonspecific outcomes. Until the development of cyclosporine 0.05% (Restasis, Allergan, Inc.), little pharmaceutical development existed. Due to the interest in dry eye being relatively recent, our current treatment armamentarium is limited compared with other ocular diseases.
To find a statistically significant difference for a treatment, intervention requires objective data that have been extremely difficult to acquire, until recently. To introduce a new treatment option into the market, the modality (whether pharmaceutical or procedural) must show a significant objective improvement in the condition being treated. Despite subjective and anecdotal evidence for some potential interventions, this has been a difficult goal to achieve for the developers of many new dry eye/MGD products.
ADVANCES IN DIAGNOSTIC TESTING
Tear osmolarity testing
We have struggled for years to properly diagnose dry eye, alternately resorting to subjective patient reports, the Schirmer test and fluorescein staining patterns, which are variable with low reliability and reproducibility.2 Today, diagnostic testing allows us to objectively characterize the condition and to follow the progress and response to treatment. Tear osmolarity testing (TearLab Corp, San Diego, Calif.) has offered a reliable benchmark for baseline testing as well as for following response to treatment.
Inflammadry
In addition, Inflammadry (Rapid Pathogen Screening, Inc, Sarasota, Fla.) immunoassay gives us an objective (although binary) assessment of inflammation by measuring elevations in MMP-9, giving us insight into the potential efficacy of adding an anti-inflammatory to our treatment regimen. It also helps us to determine whether an underlying inflammatory disorder, such as those resulting from allergy or contact lens over-wear, needs treatment.
LipiView
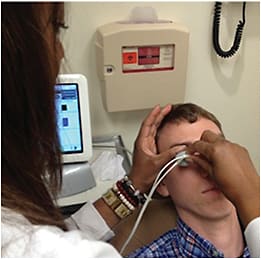
Finally, the introduction of LipiFlow and LipiView (Tear Science, Morrisville, N.C.) has allowed us to provide high-quality imaging and assessment of the dysfunctional meibomian glands. The LipiView imaging unit provides an objective measurement of the glandular function, blink rate and lipid layer thickness, as well as an imaging tool to help illustrate and discuss this dysfunction with our patients. The recent software upgrade, LipiView II, will allow us to image the meibomian glands even better than the original LipiView by adding a patented system of reflected and transilluminated light to show structure and active functioning of the glands. It allows the surgeon to customize the exam, choosing among several views of the glands, allowing the surgeon to better predict who might benefit most from LipiFlow treatment versus other treatment modalities.

Meibomian gland dysfunction with inspissated glands along the lid margin.

Meibomian gland dysfunction with debris on the base of the lashes.
ADVANCES IN TREATMENT
Manual treatment
When dealing with MGD, physicians must start with evaluating lid hygiene before initiating an appropriate treatment. This is followed by a maintenance regimen that patients can easily incorporate into their daily routine.
In our practice, we have an “MGD technician” in our “MGD clinic” who counsels patients on proper lid hygiene, trains patients to perform effective lid massage, performs manual expression and exposes patients to products such as lid scrubs, sleep goggles and cleansers.
I’ve seen impressive results with manual expression and with patient satisfaction after one-on-one counseling with a trained technician. Since these patients have often suffered long-term without any relief or empathy for the severity of their chronic condition, they find it frustrating when they perceive that a doctor can’t or won’t spend adequate time addressing their symptoms. Since one component of any chronic disease is psychological, forming an alliance with a well-trained technician dedicated specifically to educating these patients can greatly improve patient satisfaction and office efficiency. Alternatively, they may become trapped among cataract surgery pre-ops and post-ops and feel forgotten.
Supplementation
I also strongly believe in the role of omega polyunsaturated fatty acid supplementation for MGD and evaporative dry eye. I encourage all of my patients to pursue nutritional supplementation as a component of their dry eye treatment program. John Sheppard, MD, of Virginia Eye Consultants, and team recently conducted a randomized double-blind study of the effects of supplementation with omegas, which has provided some early objective data on the potential efficacy of this dry eye intervention. Specifically, they looked at the benefits of EPA (an omega-3 from fish oil) combined with GLA (gamma-linolenic acid, an omega-6 derived from black currant seed oil). Additional studies are ongoing to determine the optimal omega formulation (triglyceride or ethyl ester) and dosage regimen for supplementation.3
| TREATMENT OPTION | IMPLEMENTATION | ||
|---|---|---|---|
| Omega-3 supplementation | Dosage and formulation varies | ||
| Lid cleansers | |||
| -routine | -Ocusoft (Ocusoft, Inc.) | ||
| -demodex | -Cliradex (Bio-Tissue) | ||
| Heat/moisture goggles | Nightly | ||
| Over-the-counter lubricants | As needed, depending on severity | ||
| Doxycycline | |||
| -oral | -50-100 mg po QD to BID (GI side effects) | ||
| -compounded topical | |||
| -1 drop, 4 x daily | |||
| Anti-inflammatory/Antibiotic Combos | Steroids to be used typically for short course for control followed by non-steroid maintenance | ||
| -tobramycin/dexamethasone | |||
| -neomycin/polymixin/dexamethasone | |||
| Antibiotics (topical) | 1 drop 2 x daily for 2 days and then once daily | ||
| -azithromycin | |||
| Anti-inflammatory (topical) | 1-4 times daily with taper, depending on severity | ||
| -loteprednol | |||
| Manual expression | Every 2 months on average, depending on severity | ||
| LipiFlow thermal expression | Every 6 months, depending on severity | ||
The LipiFlow treatment uses a thermal pulsation system, a minimally invasive technique that massages the oils from the meibomian glands.
HEAT TREATMENTS
LipiFlow
We have used the LipiFlow unit for our patients over the past year with excellent results. The LipiFlow thermal pulsation system is a 13-minute, minimally invasive treatment that uses heat massage to milk the oils from the meibomian glands. It may take several weeks to experience relief from treatment. However, after one LipiFlow treatment, many patients are able to maintain the treatment effect by continuing warm compresses on their own.
MiBo Thermoflo
Another heat treatment option for patients with MGD is MiBo Thermoflo (Aesthetic Solutions, Inc., Lafayette, Colo.), which uses a thermoelectric heat pump to liquefy the meibum and facilitate expression of gland secretions. The heat is applied to the outside of the lids with an ultrasound gel breaking down the hardened material inside the glands. Treatment is recommended every two weeks and takes approximately 10 to 12 minutes per eye.
RELATED CONDITIONS
Rosacea blepharitis
Care should be taken to diagnose other related conditions that may be exacerbating the MGD, such as rosacea. Rosacea blepharitis is common and responds well to treatment with oral doxycycline. We generally begin at a dose of 50 to 100 mg twice daily for a week followed by once daily for at least a month. Gastrointestinal side effects are common; patients should be warned as the dosage may need to be adjusted accordingly if symptoms occur. In the case of side effects, topical preservative-free doxycycline drops can be formulated. These are effective in patients with moderate to severe disease.
Along with the therapeutic anti-inflammatory and anti-bacterial effects of doxycycline, pulsed-light therapy has also shown efficacy for dry eye symptoms associated with rosacea blepharitis and associated MGD in this group of patients.
Demodex
An attending physician once advised me, “What you aren’t aware of, you’ll never be able to diagnose and treat.” I’ve found this maxim particularly useful in the case of demodex. The patient response to seeing her or his eyelashes teeming with demodex organisms is an exceptionally motivating factor for compliance.
Cliradex towelettes (Bio-Tissue, Inc., Miami, Fla.) or other products made from other forms of tea tree oil, or a combination, can help eradicate this infection; however treatment generally requires at least two months for full resolution. Cliradex is a well-tolerated form of tea-tree oil, which can be used as routine lid hygiene for MGD patients even without active demodex infection. At our facility, the MGD technician performs Cliradex treatment and instructs the patient on how to use it at home. They apply the formulation onto the lashes, close to the base using a bristle brush applicator to remove debris from the lashes. At home, patients perform their treatments along with regular follow-up appointments for repeat evaluation and to cultivate a supportive relationship with the technician.
| INTERVENTION | CODING/BILLING | |
|---|---|---|
| 1. | Tear Osmolarity Testing | 83861 – RT, LT (bill eye individually)
(Medicare rate $22.71/eye) |
| 2. | LipiView/LipiFlow | Self-pay
(charge approx. $2000 with follow-up for 2 eyes) |
| 3. | MiBo | Self-pay
(charges range from $200-$500) |
| 4. | Inflammadry
(Rapid Pathogen Screening) |
83516QW (effective 02/27/14)
(average reimbursement $10.50) |
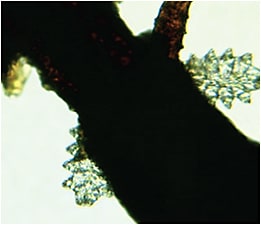
This image shows demodex organisms on an eyelash.
A SUPPORTIVE RELATIONSHIP
Cultivate dedicated staff
Despite all the advances in diagnosis and treatment, I strongly feel that part of the treatment for any chronic condition, such as MGD, is the development of a supportive relationship. Patients needs to understand that dry eye is a chronic condition and that they need to play an active role in their treatment and not see themself as a victim. Patients need to understand there is no instant fix to their problem and to pay attention to environmental triggers and perform long-term lid hygiene maintenance.
Unfortunately, with all the pressure to see more patients in a timely manner, the physician often does not have time to cultivate such a relationship. In fact, a dedicated technician actually can do a better job with this, anyway.
A rewarding experience
Even though MGD was not the initial stimulus enticing me to pursue ophthalmology, the advances in diagnosis and treatment of evaporative dry eye has given me a new appreciation when treating these challenging patients. OM
References:
1. Lemp MA, et al. Distribution of aqueous deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea. 2012;31:472-478.
2. Sullivan BD, Crews LA, Sonmez B, et al. Clinical utility of objective tests for dry eye disease: variability over time and implications for clinical trials and disease management. Cornea. 2012;Sep;31:1000-1008.
3. Sheppard JD, Singh R, McClellan AJ, et al. Long-term supplementation with n-6 and n-3 PUFAs: a randomized double blind clinical trial. July 2013. http://www.ncbi.nlm.nih.gov/pubmed/23884332. Accessed Nov. 25, 2014.
About the Authors | |

| Kendall E. Donaldson, MD, MS is associate professor at the Bascom Palmer Eye Institute, where she specializes in cornea/external disease and cataract/refractive surgery. She is medical director of the Bascom Palmer Eye Institute in Plantation, Fla.
|

| Kendra Davis, COA is a senior ophthalmic technician for the Ocular Surface Center of Excellence at Bascom Palmer Eye Institute. Ms. Davis is the only PROSE Technician in Florida and a clinical therapy technician specializing in meibomian gland dysfunction and dry eye syndrome. |