







Flatten the femto-phaco learning curve
This step-wise process can get you up to speed quickly with ReLACS.
By Kendall E. Donaldson, MD, MS
| About the Author | |
|---|---|

|
Kendall E. Donaldson, MD, MS, is associate professor at the Bascom Palmer Eye Institute, Miami. |
Fortunately for us cataract surgeons, the transition from traditional phacoemulsification to refractive laser assisted cataract surgery (ReLACS) involves a rapid learning curve, particularly when compared with the transition from extracaopsular cataract extraction to phaco.1-4 Multiple reports have documented this learning curve when incorporating femtosecond cataract technology into practice, describing a slightly higher incidence of complications during early cases.2,3
The learning curve has flattened significantly as software upgrades and better patient interfaces have made the procedure safer, more efficient and easier to perform. This article offers an approach on adopting ReLACS into practice and shortening the learning curve to achieve optimal outcomes earlier in your experience.
CHOOSE THE RIGHT CANDIDATES
Complications of ReLACS early in a surgeon’s experience include anterior capsular tears (0.31% in experienced users vs. 4% in early cases), posterior capsular tears (0.31% vs. 3.5%) and posterior lens dislocation (0% vs. 2%).2 Choosing the perfect candidates for your early cases will help ease the transition.
Patients who will be cooperative with positioning and fixation — those who display minimal anxiety and are non-claustrophobic — will be easier to dock. Those who can lie flat (no kyphosis or neck problems) will be easier to position under the laser. A well-dilated pupil will also make early cases much easier. Avoid patients with poor exposure, small orbits, prominent brows or limited cooperation (squeezing lids or inability to remain still) early on.
Later, you can progress to more complicated cases including smaller pupils (with or without Malyugin rings), hypermature cataracts, pseudoexfoliation syndrome with zonular weakness and possibly posterior polar cataracts.
STEPS IN THE FEMTO-PHACO PROCESS
Docking
For surgeons who have performed femtosecond LASIK surgery, the docking process (Figure 1) will seem quite familiar. However, even those surgeons new to laser technology find docking on all four available platforms relatively easy with most patients.

Figure 1: The docking process for femto-phaco is similar to that for femto-LASIK.
The four available laser platforms have varying patient interface systems: contact systems, which include LenSx (Alcon, Fort Worth, Texas) and VICTUS, (Bausch + Lomb, Mission Viejo, Calif.); and noncontact systems, which include Catalys (OptiMedica, Sunnyvale, Calif.) and LensAR (LensAR Inc., Orlando, Fla). Contact, or corneal applanating, systems tend to have a smaller diameter and may fit a smaller orbit better. Non-contact devices, besides causing a lower rise in IOP than contact systems, also cause less subconjunctival hemorrhage and offer a wider field of view.
Capsulorhexis
The capsulorhexis is much easier with femtosecond technology than traditional phacoemulsification. A default of approximately 5 mm diameter creates a perfect, continuous capsulorhexis 99% of the time with most platforms (and the latest software upgrades), allowing us to be precise with lens centration. This is especially important with the premium IOLs.
Occasionally, we may observe a capsular tear or irregularity, so I recommend removing the capsule with Utrata forceps in a curvilinear motion to avoid any progression of a radial tear. Some surgeons, once they are familiar with this technique and are confident the capsule is freely floating within the anterior chamber, choose to simply remove the capsule with the phaco handpiece. However, I strongly caution against this initially.
You can decrease the capsulorhexis diameter with small pupils (Figure 2). However, application of laser energy in close proximity to the pupillary border may induce pupillary miosis and floppy iris syndrome, so be cautious with these cases early in the learning curve.
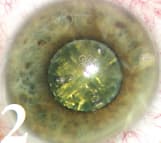
Figure 2: Small pupils, as seen here, can present possible risks of pupillary miosis or floppy iris syndrome for laser-surgery beginners.
Hydrodissection
Hydrodissection is slightly modified to allow the release of gas bubbles trapped behind the lens. Failure to release these trapped gas bubbles has been reported to cause posterior capsular rupture in rare cases.5,6 Gently tapping on the lens or tilting it slightly with the hydrodissection cannula brings the bubbles forward quickly to allow them to escape. More experienced surgeons sometimes omit hydrodissection altogether and instead release gas bubbles during the initial nuclear crack. I do not advise doing this during early cases.
Lens fragmentation
You can perform lens fragmentation (Figure 3) in various patterns according to your preference and lens density. Each platform offers several patterns of fragmentation with varying degrees of softening (chops, cubes or cylindrical subdivisions) designed to reduce necessary ultrasound. Increasing nuclear softening may significantly lengthen the duration of laser treatment, which may in turn induce pupillary miosis in some cases, particularly those with marginal pupils at the outset.
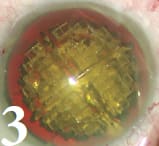
Figure 3: This image shows nuclear fragmentation under the operating microscope following the completion of femtosecond laser treatment.
MAKING CORNEAL INCISIONS
Programming incisions
The surgeon programs the clear corneal incision according to his or her preference. Some challenges associated with making the incision include its close proximity to the limbus, particularly with a liquid optics interface. If the wound is too central, it will result in more wound manipulation during phacoemulsification, increasing the propensity for wound leakage and potentially inducing more astigmatism. If the wound is too peripheral, it may involve limbal tissue, which may make it more difficult to open.
Because of these challenges, some surgeons continue to create their own manual incisions, using the femtosecond laser only for creating the capsulorhexis and softening the lens. Docking centration is also crucial for this step, because decentration can dramatically alter the placement of astigmatic incisions. When applying the patient interface, take care to avoid any cyclotorsion, which could rotate the axis of incision placement.
As with manual limbal-relaxing incisions (LRIs) and toric lens alignment, I recommend placing limbal markings with the patient in an upright position before surgery. These marks can then help properly align the treatment during docking and imaging. Upcoming iris registration software will hopefully make this process easier and ensure perfect alignment every time.
Opening incisions
Ease of opening incisions varies among the platforms. Incisions created with contact applanation lasers (LenSx and VICTUS) may be easier to open with a blunt instrument, whereas incisions with the liquid optics interface may require a blade at times. LRI nomograms are still being generated for femtosecond cataract surgery.
You can open LRIs intraoperatively or postoperatively for up to several months following the surgery. Most surgeons are waiting to open the LRIs and base their decisions on postoperative refractive error and topography. Often, the LRIs do not need to be opened.
Laser-made LRIs appear to be more consistent than those created manually, so many surgeons are adapting their treatments from manual nomograms. Several surgeons have made their nomograms available for widespread use while we gain more experience and learn new ways to customize our own nomograms. For instance, Eric Donnenfeld, MD, created a nomogram, the AMO Donnenfeld LRI calculator (www.lricalculator.com). Similarly, Louis “Skip” Nichamin, MD, has created the “NAPA” Nomogram (www.drnichamin. com or www.lricalculator.com).
It appears we can make these incisions at approximately 70% of the arc length with the laser and achieve similar or better effect compared to manual technique. They are generally made at a 7- to 9-mm optical zone and 80% corneal depth.
Some laser platforms offer the option to place these incisions on the surface or at an intrastromal location. Hopefully, in the next year or so, femto-specific nomograms will be available to help guide us with these decisions.
TRANSITION AND LOGISTICAL CHALLENGES
Phacoemulsification
If you choose to form an initial groove, generally very little manipulation is required to separate the fragments (Figure 4). Depending on the degree of lens softening, you can remove the nuclear material, often with a fraction of the ultrasound that you would need during a traditional case. You may then proceed with either a modified divide-and-conquer or chop technique.
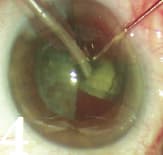
Figure 4: In laser surgery, generally little manipulation is required for nuclear fragmentation (seen here).
Working out the financials of ReLACSA femtosecond laser costs between $400,000 and $550,000, excluding the service cost after the first year, which can range from $40,000 to $50,000 a year. Disposable interface costs range from $300 to $450 per eye. In addition, other costs associated with incorporating this technology may include office or surgery center construction and hiring of new personnel. Recently, companies have begun to mobilize these platforms and bring the laser to the individual surgeon, which may provide surgeons with an opportunity to assess their practice’s response to the new technology before investing in their own laser, as well as giving a surgeon the chance to see if the technology will be cost effective in his or her practice setting. |
Cortical removal
During your early cases, cortical removal (Figure 5) in femto-phaco may be more difficult than traditional cataract surgery. The edge of the cortical sheet is typically very clean, with no tags or irregularities. Often, we perform less hydrodissection during femto-assisted cases, so the cortex may be more adherent, particularly at the subincisional cortex. Ease of cortical removal quickly improves with further experience.

Figure 5: Cortical removal (seen here) may be more difficult in laser procedures. The cortex may seem more adherent to the capsule.
WHERE TO PLACE THE LASER
Placement depends on space and laser type
Additional space, time and staff are necessary to incorporate the laser into your practice. The laser companies are more than happy to assist with training of staff and surgeon, and they are accessible for technical and engineering support (which may vary depending on the laser manufacturer and accessibility to local support personnel).
The location within the office of the femtosecond laser for cataract surgery directly impacts patient flow and volumes. Two basic models currently exist: laser in or out of the OR (in a separate room). Whether or not the laser has an integrated bed significantly impacts the size of the laser footprint and space requirements.
Inside the OR
The advantages to having the femtosecond laser in the OR include patient convenience and the ability to create full-thickness corneal incisions without the hypothetical concern of anterior chamber instability during patient transport. However, this model has the potential to slow down a busy surgical day because it ties up the OR during the FSL procedure, not allowing a conventional surgery to take place at that time.
Outside the OR
In this model, the femtosecond laser should be in a clean room similar to a refractive surgery suite, but it does not need to be in a sterile operating room because the corneal incisions it creates will not be entered. Multiple surgeons can utilize the femtosecond laser in rapid succession, or one femtosecond laser operator can perform this portion of the procedure for multiple surgeons in an efficient manner.ReLACS provides surgeons an exciting option to potentially improve patient outcomes and safety. The learning curve for adoption of this new technology is very rapid and associated with few complications if surgeons are aware of some minor technique modifications to ensure a successful transition.
COMPLICATED CASES
Small pupils
Small pupils may present a particular challenge for surgeons early in the learning curve. The pupil must be able to dilate sufficiently to make an adequate capsulorhexis (more than 4.5 mm). Applying laser energy may induce pupillary miosis, particularly in patients with initially marginal pupil size.
Additionally, the number of docking attempts per case (1.05 vs. 1.5) has been associated with induction of pupillary miosis (1.2% vs. 9.5%).2,3 Monitor the pupil carefully during treatment to prevent damage to the pupillary border by the laser application. This phenomenon is more pronounced in cases with a time lapse between the laser and phaco, so the standard is to complete phaco within 30-40 minutes of the laser.
In predetermined small pupil cases, you can create the incision (with the laser or manually), then place a Malyugin ring (Figure 6) before using the laser to create the capsulorhexis and fragment the nucleus. Take care to ensure strict adherence to sterility, which is easier with the laser in the OR.

Figure 6: In this small pupil case, incisions were made manually, viscoelastic was injected into the anterior chamber and a Malyugin ring was placed.
Pupillary miosis
Using an intense dilating regimen or adding atropine 1% drops has been critical in limiting the pupillary miosis problem. Alternatively, if you note significant pupillary miosis following laser application, you can place a Malyugin ring after the laser has been completed. In such cases, do not incorporate the edge of the anterior capsule under the ring, because this may induce an anterior capsular tear. Additionally, intracameral mydriatics (eg, preservative free, bisulfite free phenylephrine 1.5%) may be a useful adjunct for improved pupillary dilation.
Other challenges
The femtosecond laser is ideally designed to assist in challenging cases, such as pseudoexfoliation syndrome in which decreased energy and limited lens manipulation during extraction are beneficial. This also applies to cases of Fuchs’ dystrophy in which preserving the corneal endothelium is paramount.
The femtosecond laser has become an invaluable tool for softening dense nuclei. However, in cases involving hypermature white liquefied lens material, the liquefied capsular contents may escape into the anterior chamber during capsulorhexis formation, thus obstructing further femtosecond laser application necessary for completing the capsulorhexis or nuclear fragmentation. In such cases, you can use the femtosecond laser to create the incision and capsulorhexis. However, nuclear softening and fragmentation should proceed manually.
Traumatic cataracts may also be ideal for femtosecond laserassisted surgery, because lens softening may allow for less manipulation, thus preserving the integrity of potentially weak zonules. You should always approach posterior polar cataracts with caution. If an attachment to the posterior capsule exists, gas bubbles may escape posteriorly propagating a posterior capsular tear. OM
REFERENCES
1. Nagy Z, Takacs A, Filkorn T, Sarayba M. Initial clinical evaluation of an intraocular femtosecond laser in cataract surgery. J Refract Surg. 2009;25:1053–1060.
2. Sutton G, Bali SJ, Hodge C. Femtosecond cataract surgery: transitioning to laser cataract. Curr Opin Ophthalmol. 2013;24:3-8.
3. Bali SJ, Hodge C, Lawless M, Roberts TV, Sutton G. Early experience with the femtosecond laser for cataract surgery. Ophthalmology 2012;119:91-899.
4. Roberts TV, Lawless M, Bali SJ, Hodge C, Sutton G. Surgical outcomes and safety of femtosecond laser cataract surgery. A prospective study of 1500 consecutive cases. Ophthalmology 2013; 120:227-233.
5. Yeoh R. Hydrorupture of the posterior capsule in femtosecondlaser cataract surgery. J Cataract Refract Surg. 2012;38: 730; author reply 730.
6. Roberts TV, Sutton G, Lawless MA, Jindal-Bali S, Sutton G. Capsular block syndrome associated with femtosecond laser-assisted cataract surgery. J Cataract Refract Surg. 2011;37:2068–2070.