







CXL: The Great Epi-on vs. Epi-off Debate
As corneal crosslinking evolves, both techniques could be winners.
BY JERRY HELZNER, SENIOR EDITOR
| Q&A with Dr. Roy Rubinfeld of CXLUSA. |
|---|
|
Acting with the approval of several Investigational Review Boards (IRBs), a group of US cornea specialists who have extensively researched both the epi-off and epi-on techniques have come to believe the latter is superior for corneal collagen crosslinking. These ophthalmologists have formed a group called CXLUSA, which has evolved into an advocacy community for the epi-on procedure. Here, Roy Rubenfeld, MD, a spokesperson for the group, answers relevant questions about CXLUSA and its work. Q What led you and the other cornea specialists to form CXLUSA and what are the primary goals of the group? A Having followed the evolution and approval of CXL in all 25 EU countries by 2006, several of us cornea specialists in the United States were concerned that our keratoconus patients progressively losing vision under our care had no good treatment options to stop their vision loss when others had access to a proven effective treatment. We started with epi-off standard technique and then used both epi-off and epi-on before deciding that epi-on was preferable for most patients. After extensive research, we set up a physician-sponsored group to enable us to provide this treatment on an investigational basis with IRB approvals. We have presented dozens of abstracts, papers, talks on our research at AAO, ASCRS, ESCRS, ARVO and many other US and international meetings, and have been able to help many patients prevent further loss of vision and avoid corneal transplantation. Q How long has CXLUSA been in existence? A It started with one center in late 2009. Q How many ophthalmologists are part of CXLUSA? A We now have approximately 30 investigators at a small number of centers across the United States. 
The “epi-off” method of collagen crosslinking illustrated here first saturates the cornea riboflavin. Q When you formed CXLUSA, did you all have experience in performing both epi-on and epi-off crosslinking procedures? A Yes. In fact we started with the standard Dresden epi-off protocol, which had been the most extensively studied technique for crosslinking. Encouraged by the work of others, in May 2010 we started performing epi-on CXL procedures. Q Was your initial purpose to promote the potential of epi-on or were you more interested in compiling research that might prove the relative advantages and disadvantages of epi-on and epi-off? A Initially, we were very skeptical of epi-on CXL based on some early lab work out of Germany. Since CXLUSA is not an FDA trial, we were able to rewrite and modify our protocols and techniques as we gained experience and learned. We found that we were, in fact, able to obtain rapid, consistent epi-on loading and excellent clinical results by developing several innovations. We have evolved to our current techniques and protocols, which permit rapid visual recovery (usually return to work the next day), and excellent stabilization of corneal curvature with our current epi-on approach. Q You have published some three- and six-months findings showing epi-on to have better outcomes. What sort of scientific rigor have you used to validate those findings? Do you have controls in such areas as age of patients and whether progression was seen? Is six months enough time to draw a conclusion? A I can share that our failure rate is approximately 1% since May 2010, which compares favorably with Dr. Theo Seiler’s paper describing a 5% failure rate with epi-off CXL.1 We have followed many of our patients now for almost three years. Based on the extensive body of literature demonstrating the efficacy of CXL worldwide, we decided not to have controls in our studies whose vision would be expected to worsen during the study. Q What is your response to the assertion that leaving the epithelium on blocks riboflavin, oxygen and UV light needed to get the full benefit of crosslinking? A Depending on the degree of riboflavin loading of the epithelium, there can be some absorption of UV-A light application however, even at the low original “Dresden Protocol” 3.0 mw/cm2 irradiance, UV transmission to the stroma is much more than sufficient and UV-A irradiation is not the rate-limiting factor. That rate-limiting factor is oxygen and our proprietary technology is especially designed to maximize molecular corneal oxygen and collagen crosslinking while minimizing hypoxia during the procedure. Hypoxia can result in high corneal levels of peroxides in addition to other toxins. In short, the physics, chemistry and our long-term clinical results demonstrate clearly that our epi-on techniques are highly effective and provide more rapid visual recovery with reduced risk by leaving the epithelium in place in a less-invasive procedure than epi-off CXL. It is interesting that Avedro has purchased an epi-on riboflavin solution patent and will soon initiate epi-on trials in the United States. Q Is it encouraging to your group that Avedro plans to begin an epi-on clinical study? A Based on our long-term results, we believe epi-on is generally the preferred approach to crosslinking for ecatasia due to its rapid recovery, improved comfort, reduced risks, and therefore we are happy to see others study this as well. Q Do you see room for both epi-on and epi-off based on the individual case? Epi-on for milder cases? A Actually, we believe epi-on is likely to be the preferred option for CXL as a standalone procedure in nearly every case with similar efficacy and improved safety. As with other surgical procedures, the non-invasive approach has inherent safety and comfort advantages Reference1. Koller, T, Mrochen, M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract & Refractive Surg 2009: 35: 1358-1362 
Uniform stromal riboflavin visible after 15 minutes of loading in epi-on procedure. |
Already well-established in Europe for more than a decade, it is widely expected that the corneal collagen crosslinking treatment for keratoconus and post-LASIK ectasia, sometimes called CXL for short, will receive FDA approval sometime in 2014. With the 512-patient multicenter US trial complete and the data collected and analyzed, essentially all that remains for trial sponsor Avedro Inc. is to submit its application for approval to the FDA.
The effectiveness of the CXL procedure is indisputable, but a debate has erupted over whether it should be performed with the epithelium on or with the epithelium off. In one corner stands Yaron Rabinowitz, MD, of Beverly Hills, Calif., a corneal specialist and fierce proponent of performing CXL with an epi-off technique. Dr. Rabinowitz has received National Institute of Health funding continuously since 1993 for his research on keratoconus. In the other corner stands a group of cornea specialists who have formed CXLUSA to advance the less-proven epi-on form of the procedure. The leading spokesperson for this group is Roy Rubinfeld, MD, of Chevy Chase, Md.
Ask David Muller, PhD, the CEO of Avedro, about the major personalities in the epi-on vs. epi-off debate and he pauses for a moment before responding.
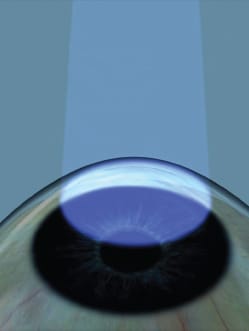
A precisely timed beam of ultraviolet-A light is applied to strengthen mechanical properties of the cornea.
“Well, you have two very passionate people there. I’m sure they’ll have no trouble making their views known.”
“This is one of the hottest debates in ophthalmology right now,” offers Salim Butrus, MD, a Washington, D.C., corneal specialist.
The Basic CXL Procedure
No one disputes the effectiveness of the basic CXL procedure, which is designed to strengthen the cornea and actually reverse the visual deficits keratoconus and post-LASIK ectasia cause. Currently, the procedure can be successfully used in patients with minimum corneal thickness of 400 μm and no other contraindications such as a history of herpetic infection or corneal scarring. For many patients, CXL is the only procedure that can allow them to avoid a corneal transplant.
In its simplest terms, CXL first saturates the cornea with riboflavin, followed by the precisely timed application of a beam of UV-A light to strengthen the mechanical properties of the cornea. Avedro, which is expected to dominate the CXL field in the United States when the procedure is approved, provides the equipment and supplies for performing the procedure. The company has also shepherded CXL through the clinical trial process.
The Great Debate
Though Avedro has experimented with ways to shorten the time required for the procedure, it has been diplomatic in not taking sides in the epi-on vs. epi-off issue.
The data it will submit to the FDA will be based solely on the more-proven epi-off procedures. However, Dr. Muller told Ophthalmology Management the company will soon begin a new crosslinking trial employing the epi-on technique.
“As of today, this minute, we believe the epi-off technique produces superior results,” says Dr. Muller. “This is because taking the epithelium off allows more riboflavin, more UV light and more oxygen to permeate the cornea. In other words, leaving the epithelium on presents a barrier to obtaining the full effect of the procedure. But the epi-on technique offers more comfort to the patient, and it can be improved. So what is true today won’t necessarily be true a year from now, or five years from now. What is needed is a controlled study of epi-on, and we plan to do that.”
Peter Hersh, MD, of Teaneck, N.J., is the medical monitor for Avedro. He has been involved in numerous CXL studies and is generally considered an authority on the procedure.
“The first thing you have to understand is that crosslinking is a new technology that is growing and evolving,” he says. “The epi-on vs. epi-off debate is interesting, and it makes for a good story, but in the long run we may see a number of different techniques being used for a variety of indications. We shouldn’t assume that we will see a winner and a loser. I definitely don’t see it that way.”
The epi-on technique has three major hurdles to overcome, Dr. Hersh notes: saturation of the cornea with adequate riboflavin; eliminating the blockage of UV-A light; and allowing the level of oxygen concentration so critical to the success of the procedure. “The epi-on people have been working on overcoming these obstacles,” he says. “I believe they have had success in the area of riboflavin saturation. I’m sure they are working on all aspects of the procedure.”
Other Avedro CXL Initiatives
Besides the basic CXL procedure, Avedro has under way a major initiative called LASIK Xtra that uses riboflavin and UV-A light to strengthen the cornea as part of a LASIK or PRK procedure. Avedro says the few extra minutes LASIK Xtra requires pose no material interruption to the normal speed and flow of the LASIK procedure itself and does not increase patient discomfort. The company believes that the strengthening of the cornea provided by LASIK Xtra may be applicable to all current LASIK patients, and cites approximately 50,000 LASIK Xtra procedures already performed worldwide.
Slit-lamp photo of riboflavin loading during epi-on CXL shows good saturation.
Avedro also says it has made a breakthrough discovery that reduces crosslinking time from one-hour to three minutes or less, although that will not be part of its initial FDA approval application. Avedro says its KXL System for Accelerated Cross-linking achieves speed by increasing the UV-A power and reducing the exposure time, maintaining the same energy on the eye as standard crosslinking while reducing crosslinking time by an order of magnitude.
Finally, Avedro has initiated a partnership with Eye Gate Pharmaceuticals to determine if Eye Gate’s method of delivering ophthalmic drugs through a process called iontophoresis (essentially via a small electric charge) would be feasible for delivering riboflavin in an epithelium-on technique. OM
| Q&A With Yaron Rabinowitz, MD. |
|---|
|
Q You have been acknowledged as one of the country’s leading experts on the treatment of keratoconus and the epi-off method for CXL, receiving continuous NIH research funding for two decades. What are the key reasons why the epi-off technique is superior? A To answer this question, lets look at the published data: In 2009, Gregor Wollensak, one of the originators of the Dresden crosslinking technique, performed laboratory experiments performing CXL on three groups of animal eyes:1 group 1, standard epi-off technique; group 2, epi-on with a benzalkonium chloride-containing proxymetacaine eyedrops to disrupt the epithelium to allow stromal penetration of riboflavin; and group 3, epi on with preservative-free anesthetic. He found that biomechanically group 2 had about 20% of the effect of group 1, and that Group 3 showed no effect at all. In 2012, Carina Koppen et al. from Belgium did a study on 53 eyes with the epi-on technique using proparacaine drops 0.5% preserved with BAC 0.005% to disrupt the epithelium and allow riboflavin penetration.2 At 12 months, they found continued progression of their keratoconus. In a recent confocal microscopy study of corneas following collagen crosslinking, David Touboul and Joseph Colin from France found that transepithelial CXL did not appear to alter corneal morphology.3 However, they found significant changes following the standard epi-off technique. In the past year, with more than 100 published articles on corneal collagen crosslinking for keratoconus, only two articles appeared to suggest that epi-on may be effective. So if you are data-driven, which I am, it would be hard to make an argument for the effectiveness of the epi-on procedure. The scientific data also supports what we have seen in our clinic. In the past several years, we have seen more than 30 patients who progressed, some very rapidly, despite the epi-on procedure. With more than 300 patients who were progressive done in our own practice to date, we have only seen two patients whom we think might have progressed by 0.50 D. Though as our study goes out longer, we would expect this number to increase slightly based on the long-term follow up reported from the European studies. Q Avedro says CXL is an evolving procedure and you, yourself, have found better results by using a laser to remove the epithelium. Isn’t it possible that the advocates of epi-on can also find ways to improve their technique? A There is no doubt in my mind that CXL is an evolving procedure and there may be ways to get the riboflavin adequately and homogeneously into the stroma without removing the epithelium. Iontophoresis is one such technique that is currently being studied. We are using a technique to remove the epithelium, which is advantageous to the patients receiving this treatment, making keeping the epi-on a moot point in our opinion. We remove the epithelium with the excimer laser using the phototherapeutic keratectomy (PTK) mode. This idea was first floated by George Kymionis in Greece in which he demonstrated that by using this technique, his patients immediately had a 2-line improvement in visual acuity. Subsequently he reported on 38 patients in the journal Ophthalmology in which he compared 19 patients using the manual epi–off technique to 19 patients with the PTK removal technique and he found that after one year these patients all saw better with no long term consequences.4 At last year’s ASCRS meeting, Bruce Jackson’s group from Canada reported a similar experience with decreased spherical equivalent and improved acuity; this was subsequently published in the Canadian Journal of Ophthalmology.5 We have used this technique on more than 100 patients, and it is our preferred technique for removing the epithelium. We presented our data on approximately 90 eyes at this year’s ASCRS meeting. Not only have we noted and improvement in acuity, but the steepest K-reading is much flatter than with conventional mechanical techniques. This allows for much-improved comfort in contact lens fitting after the crosslinking procedure. Q CXLUSA has released data that asserts their epi-on outcomes are superior, with fewer failures. How would you characterize the rigor of their data? A I have not seen any peerreviewed publication or scientific presentation of their data that would support the claim that their outcomes are superior. Since much of what they do they claim is proprietary, it would be difficult to reproduce or scientifically support what they are suggesting. I think that unless they publish their data in a peer-reviewed manuscript so that it can adequately be evaluated and reproduced by others, or present scientifically reproducible data at one of our scientific meetings, they will continue to have a credibility issue. Q Do you foresee a time when both epi-off and epi-on will be accepted techniques based on the individual patient and the type of indication? A Yes, this situation already exists. In some patients with very thin corneas, epi-on might be better despite less efficacy, as well as in some pediatric situations where the child may be difficult to manage with the epi-off technique. In the future, we might also want to do this technique in young patients with very mild or forme fruste keratoconus so as not to expose them to the risks of the epithelial defect. These potential indications will evolve as we continue to learn more about this procedure. Q How do you see most CXL being performed five years from now? Is epi-off going to be the standard technique? A Difficult to know. If increased efficacy and comfort can be demonstrated with newly developed epi-on techniques, this might be what patients choose. It certainly is more appealing to them. Based on what I know now, I prefer our technique using the PTK mode since not only do we halt the progression, but also provide a benefit of improved vision and improved contact lens comfort. I can also see a time when in addition to the PTK, we will routinely try and reduce the cylinder (removing very little tissue) with the excimer laser in older patients whose corneas are not too thin to give them an even better visual outcome following CXL. Q In Europe, where CXL has a long history of success, do you see any interest from those European ophthalmologists in doing the epi-on procedure? A At a recent ESCRS symposium on collagen crosslinking in Milan attended by more than 200 physicians, the moderator asked the group if anyone was doing epi-on crosslinking. Not a single person put up their hand. Remember, most of these docs have been doing this procedure for over a decade already. So I do not get the feeling there is a high interest in Europe or even that the Europeans believe that epi-on works. Q Just how great a barrier to a successful procedure is leaving the epithelium on? Most doctors who have performed both epi-off and epi-on see the blocking of riboflavin, UV-A light and oxygen by the epithelium as substantial hurdles to overcome. A The epithelium is a barrier to the riboflavin getting into the corneal stroma. That is why in the Dresden technique the epithelium is removed in its entirety. This allows homogenous soaking of the stroma by the riboflavin. For crosslinking to occur, there must be an interaction between the riboflavin and the UV light. In most epi-on procedures, a substance is added to disrupt the tight junctions of the epithelial cells to potentially allow the riboflavin to overcome this barrier and enter the corneal stroma. Q Do you see actual dangers to the patient in doing the epi-on procedure? A I do see two potential dangers: First, offering this procedure to a patient with the hope that it will halt the progression. Then, the progression occurs anyway because of lack of efficacy of the procedure when the patient did have access to a more efficacious procedure at that time. If the cornea was not soaked homogeneously, the UV light would bypass the areas where there is no riboflavin and damage the endothelium or lens. I am not an expert on UV light so I don’t know what the potential consequences are of this amount of UV light going to the back of the eye, but this is a big concern for me. OM References1. Wollensak G, Iomdina E. Biomechanical and histological changes after corneal crosslinking with and without epithelial debridement. J Cataract Refract Surg. 2009;35:540-546. 2. Koppen C, Wouters K, Mathysen D, Rozema J, Tassignon MJ. Refractive and topographic results of benzalkonium chloride-assisted transepithelial crosslinking. J Cataract Refract Surg. 2012;38:1000-1005. 3. Touboul D, Efron N, Smadja D, Praud D, Malet F, Colin J. Corneal confocal microscopy following conventional, transepithelial, and accelerated corneal collagen cross-linking procedures for keratoconus. J Refract Surg. 2012;28:769-776. 4. Kymionis GD, Grentzelos MA, Kounis GA, Diakonis VF, Limnopoulou AN, Panagopoulou SI. Combined transepithelial phototherapeutic keratectomy and corneal collagen cross-linking for progressive keratoconus. Ophthalmology. 2012;119:1777-1784. 5. Kapasi M, Baath J, Mintsioulis G, Jackson WB, Baig K. Phototherapeutic keratectomy versus mechanical epithelial removal followed by corneal collagen crosslinking for keratoconus. Can J Ophthalmol. 2012;47:344-347. |