







Corneal Inlays and the Presbyopic Patient
Although still investigational in the United States, corneal inlays have the potential to treat millions of presbyopes.
BY ROGER STEINERT, MD
Attempts to treat presbyopia have ranged from the simple nonsurgical spectacle or contact lens to the more involved surgical lens-based procedures such as accommodating or multifocal IOLs, or corneal-based procedures such as PresbyLASIK or conductive keratoplasty. Scleral expansion hasn’t achieved significant market penetration and most surgeons don’t use the technique.
Under investigation in the United States (and approved in many countries outside the United States) is a corneal intrastromal approach with inlays.
The concept behind corneal inlays has been explored since the 1960s; J.I. Barraquer is credited as the original innovator.1 Decentration, ketrolysis and opacification were common issues with the earliest iterations. Today’s inlays, however, are highly biocompatible, with a very thin profile and small diameter. The surgical techniques used to insert these inlays began with microkeratomes and now largely utilize femtosecond lasers to create the tunnel or flap under which the inlay is placed. All inlays are designed for implanting in the non-dominant eye to correct for near vision while using the dominant eye for distance vision. The procedure is reversible, if necessary, and the surgical implantation technique itself is fairly simple.
The three inlays under commercial development are the KAMRA (AcuFocus), the Raindrop (ReVision Optics) and the Presbia Flexivue Microlens (Presbia).
Using the Femtosecond Laser
When surgeons began using inlays, we used femtosecond lasers to create flaps, much like we would for LASIK. With LASIK, however, surgeons have become rather adept at creating thin flaps; with the inlays, we need to target a 160-micron depth. The primary reason for that depth is to allow nutrients to migrate around the inlay. However, one study has indicated a flap depth of 200 microns would be beneficial in eyes undergoing simultaneous procedures.2
As surgeons, we’ve moved from the standard LASIK flap to these thicker flaps, but I believe we’ll soon be avoiding creating a full LASIK flap at all and instead create pockets to implant these inlays.
Using the femtosecond laser to create a pocket is fairly straightforward — and each of the various femtosecond lasers commercially available can be used for this purpose. The pocket is, in essence, a “slot” that transects considerably fewer nerve endings than a full flap. Further, corneal structural integrity is maintained at a much higher rate than using a thick flap. The Flexivue Microlens changes the refractive index, the KAMRA increases the depth of focus, and the Raindrop changes the anterior corneal curvature.3 We don’t yet know if these inlays will function as satisfactorily with a pocket as they do with a full flap, and the Flexivue is currently the only inlay being investigated with a pocket-only implantation technique.3 I believe we’ll have a much clearer understanding of the implantation depth needed to achieve the best results in the next year or so.

Figure 1. A slit lamp image of the Presbia Flexivue Microlens.

Figure 2. The Raindrop inlay is virtually undetectable.
We know from the laser vision correction market that, compared to phakic IOLs, patients would rather undergo a corneal-based procedure than an intraocular one. So, a presbyopic treatment that involves the cornea is a welcome addition to our armamentarium. Once these devices are approved — and we may see the first one commercially available in the United States as early as 2014 — there will be an enormous amount of interest. From a patient’s perspective, these inlays result in zero residual impact — meaning if the inlay needs to be removed for any reason, the cornea reverts to its pre-inlay state and the patient’s optical situation reverts to pre-inlay as well.
Briefly, here are some of the differentiating points of these inlays.
The Flexivue Microlens
The Flexivue Microlens is a hydrophilic acrylic inlay that is 3 mm in diameter and has an edge thickness of about 15 microns. It received the CE Mark in Europe in 2009, and Presbia submitted an investigational device exemption to U.S. regulators in November 2012. The device should be implanted about 200 microns deep. Ioannis Pallikaris, the developer of the Flexivue Microlens, has called the entire procedure “smart monovision.” The inlay features peripheral refractive zones that range from +1.5D to +3.25D, with a neutral central zone.
The 12-month results from a post-market surveillance study4 conducted in 2011 found 78% of patients no longer needed spectacles for near vision, and patients went from an average preop visual acuity of 20/100 to 20/25-1. Within a month after surgery, binocular distance vision was 20/25 in all 40 patients.4
The KAMRA Inlay
The KAMRA is a small aperture inlay (3.8 mm in diameter) comprised of polyvinylidene fluoride (PVDF). The device uses a “depth-of-focus” similar to photography and mainly allows the fairly parallel central rays to reach the retina through the 1.6 mm fixed central aperture. The KAMRA inlay PMA has been submitted for U.S. approval, and is the first to be submitted for U.S. regulatory approval. The inlay is already approved in 48 countries across Europe, Asia-Pacific, Middle East and the Americas.
Results from a long-term study of 22 patients at 4 years post-implantation showed that patients maintained a 2+ line improvement in near vision with no significant loss in distance vision.5 In this study, a prior generation of the inlay was implanted on the stromal bed under a microkeratome-created LASIK flap (no ablation was performed). Over time, five patients developed cataracts. Four inlays were explanted during the study – two as a result of flap complications and two as a result of changes in refractive status.
Investigators in Japan are currently evaluating the simultaneous treatment of ametropia and presbyopia with combined LASIK/KAMRA implantation. In those studies, the inlay is placed under a 200 micron femtosecond-created LASIK flap once the excimer ablation is completed.2 The study enrolled 360 eyes of 180 patients with a mean age of 52.4 years ± 5.1 (SD) (range 41 to 65 years). At the time of publication, sixty-four patients were available for the 6-month postoperative examination. The mean logMAR uncorrected near visual acuity in the eye with the inlay improved seven lines in hyperopic eyes, six lines in emmetropic eyes, and two lines in myopic eyes. The mean logMAR uncorrected distance visual acuity improved by three lines in hyperopic eyes, one line in emmetropic eyes, and 10 lines in myopic eyes, respectively. Some postoperative symptoms including dry eye, halo, glare or nightvision disturbances were reported occasionally, but those are also common after LASIK surgery.
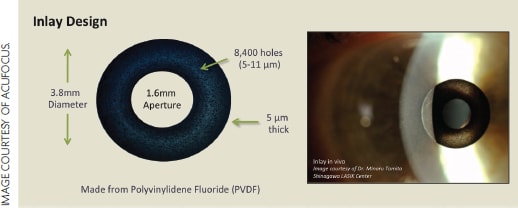
Figure 3. The KAMRA inlay.
The Raindrop Inlay
The Raindrop is a 2 mm inlay, made of hydrogel material that is about 80% water. Because it is transparent, the device does not restrict the amount of light reaching the retina. It uses a space occupying lenticule to create a hyperprolate cornea to correct near and intermediate vision. Distance acuity is minimally affected as light rays paracentral to the inlay remain focused on the retina.6 Originally, the lens was designed for implantation in emmetropic presbyopes with 20/25 or better distance vision who required between 1.5D and 2.5D of near add.
A phase 3 prospective, multicenter study evaluating the lens (under its previous name, the PresbyLens) began in June 2012. In early January, the company submitted 6-month follow-up data to the FDA from 75 of 100 patients enrolled in the first portion of the phase 3 study.7 Among the highlights: All patients had uncorrected near visual acuity of 20/25 (J1) or better in the treated eye. All subjects (100%) achieved 20/25 (J1) or better when tested bilaterally; 97% of subjects had an uncorrected intermediate visual acuity of 20/32 or better in the treated eye and 99% of subjects achieved 20/32 or better when tested bilaterally; 96% of subjects had an uncorrected distance visual acuity of 20/40 or better in the treated eye. All subjects (100%) achieved 20/20 or better when tested bilaterally; 91% of subjects gained 4 lines or more of uncorrected near visual acuity in the treated eye as measured on a standard eye chart. Patient satisfaction was high as well, with 94% citing they were “satisfied” with the correction achieved.
Some Final thoughts
From my perspective, the truly exciting aspect of corneal inlays is that we’ve been telling our LASIK patients for the past two decades that they’ll need reading glasses once presbyopia sets in. I can’t begin to guess how many of my patients shrugged and told me “you’ll come up with something by then,” and now I can tell them they were right. Most refractive surgeons will have thousands of patients who are now potential candidates for additional refractive correction.
Even patients who underwent laser vision correction with a microkeratome are potential new patients for these devices.
Once surgeons alert their patients about these devices, I think there will be an enormous amount of buzz built up quickly, in a way that’s been unprecedented in refractive surgery. ■
References
1. Barraquer JI. Modification of refraction by means of intracorneal inclusions. Int Ophthalmol Clin 1966;6(1):53-78.
2. Tomita M, Kanamori T, Waring GO IV, et al. Simultaneous corneal inlay implantation and laser in situ keratomileusis for presbyopia in patients with hyperopia, myopia or emmetropia: Six-month results. J Cataract Refract Surg. 2012;38(3):495-506.
3. Pallikaris IO, Slade S, Vukich J, Bouzoukis D. Corneal inlays for presbyopia. Presented at the 29th Congress of the ESCRS; September 19, 2011; Vienna, Austria.
4. Presbia. “Presbia announces 12-month results for Flexivue Microlens.” Press release issued November 14, 2011.
5. Yilmaz OF, Alagoz N, Pekel G, et al. Intracorneal inlay to correct presbyopia: Long-term results. J Cataract Refract Surg 2011;37(7):1275-1281.
6. ReVision Optics. “ReVision Optics Receives FDA Approval to Complete Enrollment in Its Phase III Clinical Trial with the Raindrop Near Vision Inlay for Improving Near Vision in Patients with Presbyopia” Press release issued February 25, 2013.
7. Waring GO IV, Klyce SD. Corneal inlays for the treatment of presbyopia. Int Ophthalmol Clin 2011;51(2):51-62.

Roger Steinert, MD, is the Irving H. Leopold Professor of Ophthalmology, Chair of the department of Ophthalmology and Director of the Gavin Herbert Eye Institute at the University of California, Irvine. He may be reached at steinert@uci.edu or by phone at (949) 824-8089. |