







DSEK, DSAEK & DMEK: How to Choose?
An expert explains the distinctions between three popular options for corneal grafting.
By Thomas John, MD
After relying for decades on traditional full-thickness penetrating keratoplasty (PKP)—and accepting all its attendant risks—corneal surgeons have in recent years migrated from PKP to the most advanced form of corneal transplantation currently available; namely, Descemet's membrane endothelial keratoplasty, or DMEK. The driving force behind these surgical transformations was the quest for a better and safer procedure. Corneal surgeons recognized the need for a safer surgical procedure than an open-sky, full-thickness procedure that has significant surgical downsides, including the potential for an expulsive hemorrhage and loss of intraocular contents on the operating table. Additionally, there exists the possibility of an accidental traumatic injury to the cornea with a PKP that can result in corneal wound dehiscence and potential loss of the eye, which can be devastating to any patient, and even more so in a monocular individual.
In eyes with permanent endothelial compromise resulting in suboptimal vision, if one can replace the diseased parts of the cornea and retain the healthy anterior cornea, this can be of great benefit to the patient, since we eliminate (for the most part) surgically-induced corneal astigmatism that otherwise erodes into the quality of postoperative vision following such procedures. Further, in an era of early understanding of corneal biomechanics, retaining the anterior cornea in its pre-surgical status will be of added benefit. Such an approach may be called selective corneal transplant, or SCT, where only the diseased parts of the cornea are exchanged for a corresponding healthy disc of donor corneal tissue.
However, there was no quick and easy transition to reach these ideal surgical goals until recently. The first reference in the ophthalmic literature on the subject of posterior lamellar keratoplasty (PLK) can be found in a paper written in 1950 by José I. Barraquer from Bogota, Columbia, who stated that it is “for cases of incipient endothelial dystrophies.” Barraquer's surgical technique consisted of a square anterior lamellar flap combined with resection and replacement of the posterior corneal lamellae, including the Descemet's membrane and endothelium. The anterior flap was then sutured. In 1956, Charles Tillett from Charlotte, NC published a paper in the American Journal of Ophthalmology describing his technique of PLK. These two surgeons, Drs. Barraquer and Tillett, are the true fathers of SCT. This was the first major milestone in improved corneal transplantation procedure, thus trying to move away from the full-thickness PKP procedure became a feasible goal to pursue.
However, these early surgical attempts to improve corneal transplantation were mostly forgotten until almost half a century later, when Gerrit Melles from the Netherlands started where the pioneers of endothelial keratoplasty had left off in the 1950s. In 1998 Dr. Melles showed that a surgically resected corneal disc with diseased endothelium can be replaced with a similar partial-thickness donor disc and that it can be attached to the inner corneal surface of the patient's cornea without any sutures. He used air for the initial support of the donor disc to the patient's cornea. This was truly the second milestone towards SCT.
These advances in surgical techniques led to deep lamellar endothelial keratoplasty (DLEK). Although DLEK was a huge step forward in the arena of corneal transplantation, it was not universally accepted by corneal surgeons due to the demands in the surgical skill-set to perform such a procedure on a routine basis. After simplification of the procedure with DSEK surgery, followed by DSAEK surgery, SCT became a reality for the first time and it was largely accepted by corneal surgeons worldwide. DSEK and DSAEK were then followed by DMEK.
Three Options
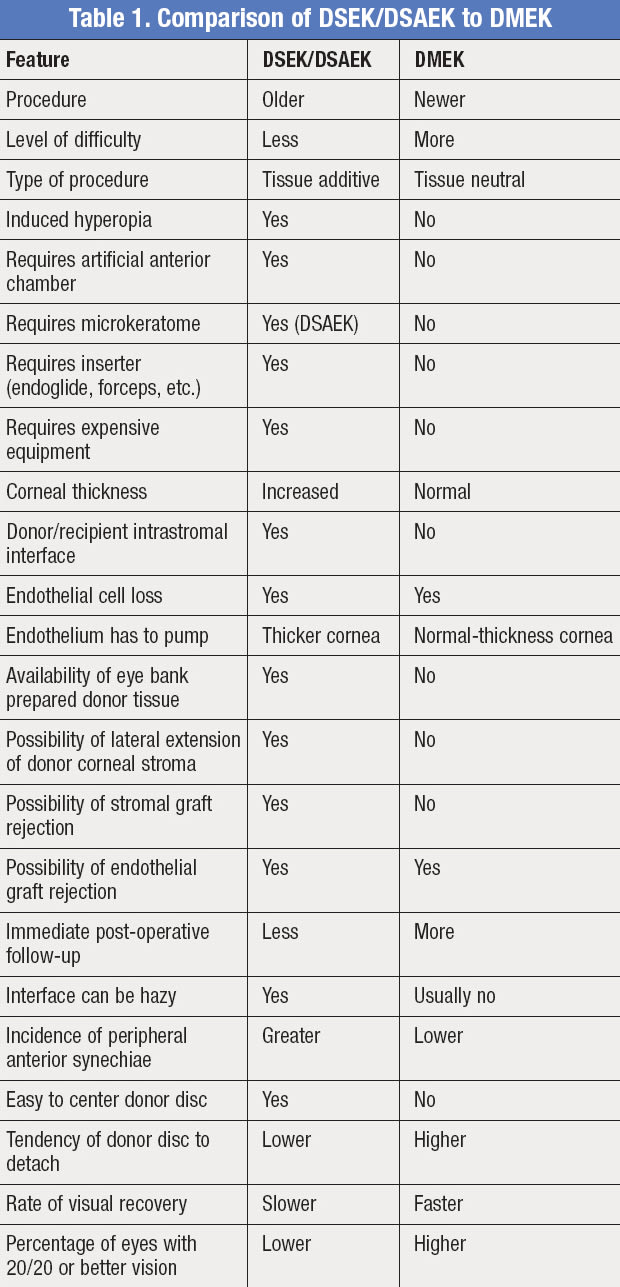
With now three viable procedures at our disposal, the question arises: which procedure should I choose for my patient with permanent corneal endothelial decompensation? To try to answer this important question, let us first briefly review these different surgical procedures. Some of the differences between DSEK/DSAEK and DMEK are shown in Table 1.
The type of anesthesia for any of the following surgical procedures can be topical with monitored anesthesia care (MAC), peribulbar injection or general anesthesia. MAC is usually the preferred type of anesthesia; however, the surgeon can choose his preferred anesthesia for the procedure.
■ DSEK. A circular mark is placed on the patient's corneal surface and it serves as a guide for removal of the recipient Descemet's membrane. The anterior chamber is entered through a peripheral stab incision, and Descemet's membrane is scored and detached as a single disc under viscoelastic. Alternatively, an anterior chamber maintainer can be used during Descemet's membrane removal. It is important not to damage the inner surface of the patient's cornea during this step of Descemet's membrane removal, since the inner corneal stroma will form half of the donor/recipient interface. An inferior peripheral iridectomy is performed to prevent postoperative air-bubble associated pupillary block glaucoma attack. Viscoelastic is completely removed from the anterior chamber using an I/A unit. It is important not to leave residual viscoelastic in the anterior chamber as it is thought to potentially hamper good adhesion between the donor corneal disc and the recipient corneal stroma.
Next, the donor cornea is mounted within an artificial anterior chamber and pressurized. Manual dissection is used to remove the anterior corneal stroma. The dissected donor corneal tissue is then placed with the epithelial side down and trephination is carried out from the endothelial side using a disposable trephine. The diameter of the trephine matches the diameter of the circular mark placed on the corneal epithelium of the recipient cornea made at the beginning of the procedure. The donor disc is about 150 microns thick.
A small amount of viscoelastic is placed on the endothelial surface of the donor corneal disc. The donor corneal disc is then introduced into the anterior chamber using a taco-fold technique using a forceps or inserted using a surgical glide or an inserter in its unfolded, or partially-folded, state. Once within the anterior chamber, the donor disc is attached to the recipient's inner corneal stroma using a large air bubble. The donor/recipient interface is formed between donor and recipient corneal stroma. The donor disc is then centered to the recipient cornea using the pre-placed epithelial circular mark. About 10 minutes is allowed to elapse to facilitate initial donor recipient corneal disc adherence. The air bubble size may be decreased at the end of the procedure. The patient is asked to lay flat in the recovery room for about 45 minutes to an hour and also to lay flat for the most part during the first post-operative day.
■ DSAEK. The surgical steps in DSAEK (Figure 1) are similar to those described above for the recipient cornea. However, the donor corneal dissection is changed from a manual approach to an automated, microkeratome-assisted procedure. Hence, the stromal interface is improved in DSAEK as compared to DSEK. This improved donor-recipient interface is thought to contribute to improved quality of vision in DSAEK. For DSAEK, precut eye bank-prepared tissue is available. This eliminates the need for surgeon preparation of the donor corneal tissue in the operating room. However, surgeon preparation of donor tissue does allow for some degree of changes in the parameters of the donor tissue in the operating room and decreases the overall cost of the procedure.

Figure 1. Slit lamp photo of a DSAEK cornea that is clear. Notice that the overall corneal thickness is increased following DSAEK.
■ DMEK. The recipient corneal dissection in DMEK (Figure 2) is similar to the above two procedures, resulting in the exposure of the patient's uncut inner corneal stroma. An inferior peripheral iridectomy is performed as in DSEK and DSAEK procedures. The donor Descemet's membrane is scored, partially detached under fluid, and trephined from the endothelial side. The Descemet's membrane with the healthy donor corneal endothelium is removed as a single donor disc without any donor corneal stroma. Hence, there is no need for an artificial anterior chamber or a microkeratome in the donor tissue preparation.
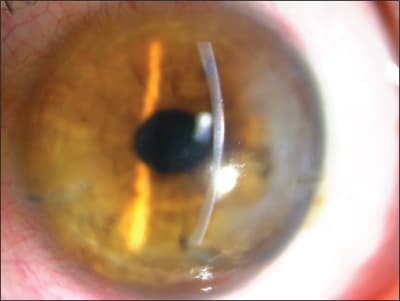
Figure 2. Slit-lamp photo of a cornea following DMEK with a clear and compact cornea.
This donor Descemet's membrane/endothelial complex is stained with a vital dye such as trypan blue for visualization. The donor disc without any stroma is then introduced into the recipient anterior chamber through a temporal wound. The default shape of the donor disc is a coiled circular tube. This donor disc is then uncoiled using fluidics, and the surgeon must avoid for the most part any direct instrument contact to the donor endothelium. Proper orientation is essential prior to attaching the donor Descemet's membrane to the exposed recipient bare corneal stroma using an air bubble. Postoperatively, the patient lies flat both in the operating room as well as at home during the first postoperative day.
How to Choose?
Having looked at the different SCT procedures for corneal endothelial transplantation, which one should I choose? It is fair to state that DSEK, DSAEK, and DMEK each appear to be superior to PKP, and hence we will not be blamed if we choose any one of these procedures for our patients.
It is wise to choose a procedure based on the experience of the operating surgeon. DMEK in its current form is a more difficult procedure than the more mature and established DSAEK surgery. The surgeon may elect not to choose DMEK if he lacks experience and the required procedure-driven surgical skills, as DMEK has the potential of accidental damage to the donor endothelium and Descemet's membrane during the surgical preparation step, with significant added cost to this surgery. DSAEK may provide a better outcome based on his skill sets relative to the procedures.
In time, learning and understanding these newer surgical techniques will facilitate the transition from DSEK/ DSAEK to DMEK without jeopardizing the surgical outcome. While DMEK appears to be a superior procedure as compared to DSEK/DSAEK and my preferred procedure, my prediction is that DMEK will undergo further transformations to a much simpler procedure, and until then DSAEK will continue to be the dominant player in SCT procedures for corneal endothelial decompensation. OM
References
1. Casey TA, Mayer DJ. Corneal Grafting. Principles & Practice. Philadelphia: WB Saunders Company; 1984;11.
2. Barraquer JI. Keratoplasty. CVI Concilium Ophthalmologicum, Britannia. 1950;(2):999.
3. Tillet CW. Posterior lamellar keratoplasty. Am J Ophthalmol. 1956;41:530-3.
4. John T. Surgical Techniques in Anterior and Posterior Lamellar Keratoplasty. New Delhi, India: Jaypee Brothers Medical Publishers; 2006:1-687.
5. John T. Step by Step Anterior and Posterior Lamellar Keratoplasty. New Delhi, India: Jaypee Brothers Medical Publishers; 2006:1-297.
6. John T. Selective tissue corneal transplantation: a great step forward in global visual restoration. Expert Rev Ophthalmol. 2006;1:5-7.
7. Terry M. The evolution of lamellar grafting techniques over twenty-five years. Cornea. 2000;19(5):611-6.
8. Melles GR, Eggink FA, Lander F, Pels E, Rietveld FJR, Houdijn-Beekhuis W, Binder PS. A surgical technique for posterior lamellar keratoplasty. Cornea. 1998;17(6):618-26.
9. Melles GRJ, Lander F, Beekhuis WH, Remeijer L, Binder PS. Posterior lamellar keratoplasty for a case of pseudophakic bullous keratoplasty. Am J Ophthalmol 1999;127:340-1.
10. Price FW, Price MO. Descemet's stripping with endothelial keratoplasty in 50 eyes: A refractive neutral corneal transplant. J of Refractive Surgery. 2005;21:339-45.
11. Busin M, Arffa RC, Sebastiani A. Endokeratoplasty as an alternative to penetrating keratoplasty for the surgical treatment of diseased endothelium initial results. Ophthalmology 2000;107:2077-82.
12. John T (Ed): The Chicago Eye and Emergency Manual. Jaypee-Highlights Medical Publishers Inc., Chapter 2, Pages 35-90, 2011.
13. Ham L, van Luijk C, Dapena I, Wong TH, Birbal R, van der Wees J, Melles GR: Endothelial cell density after descemet membrane endothelial keratoplasty: 1- to 2-year follow-up. Am J Ophthalmol. 2009;148(4):521-7.
14. Dapena I, Moutsouris K, Droutsas K, Ham L, van Dijk K, Melles GR. Standardized “no-touch” technique for descemet membrane endothelial keratoplasty. Arch Ophthalmol. 2011;129(1):88-94.
15. Price MO, Gorovoy M, Benetz BA, Price FW Jr, et al. Descemet's stripping automated endothelial keratoplasty outcomes compared with penetrating keratoplasty from the Cornea Donor Study. Ophthalmology. 2010;117:438-44.

|
Thomas John, MD, is a clinical associate professor at Loyola University at Chicago, and in private practice in Oak Brook, Tinley Park and Oak Lawn, Ill. A world leader in lamellar corneal surgery, he has edited several books on anterior and posterior lamellar keratoplasty. He can be reached at tjcornea@gmail.com. He has no financial interest in any aspect of this article. |