







Three “Rights” of Premium IOL Satisfaction
The right lens, the right education and the right questions shape outcomes and perceptions of surgery.

By Jeffrey D. Horn, MD
A common refrain in ophthalmology says that patient satisfaction after surgery depends on how we've set expectations. Did we achieve what we said we'd achieve? In my practice, where I perform both premium IOL implantation and laser vision correction, I'm not only achieving the outcomes I want for my patients, but according to ongoing satisfaction surveys, patients are highly satisfied, too. It all begins with implanting the right lens in the right patient.
The Right Lens
Patients are happiest when they have the right lens for their individual goals and lifestyle, so it's vitally important that we take the time to learn about these aspects of our patients' lives. My practice is called Vision for Life, and it's designed to educate patients about the choices available to them in lens replacement surgery so I can custom fit IOLs to patients, rather than putting the same lens in every patient. In my experience, it pays to focus on a few key principles.
Keep your treatment options open. Since I need to put the right lens in the right patient, I can't limit the lenses I use. All lenses have roles, and it's my job as a surgeon to know their benefits and limitations, their side effect profiles and how they work. I need to learn about the anatomy of a patient's eyes through corneal topography and OCT, as well as the patient's ocular pathology. Finally, I have to know how every lens will perform in helping to enhance specific visual needs and lifestyles. Together, all of this information helps me meet patients' needs, minimizing the side effects and maximizing the effectiveness of surgery and patient satisfaction. For example, my go-to lens is the Restor (Alcon), but if a patient wants the best night vision or has corneal guttata or epiretinal membrane, they'll do better with the Crystalens (Bausch + Lomb).
Explain advanced technology lenses. The majority of my patients receive advanced technology lenses such as toric or presbyopia-correcting lenses. Note that I don't call them “premium lenses,” which to me implies that they're a luxury patients don't need. Even in tough economic times, I'm implanting advanced technology lenses at least 75% of the time. I explain the advantages of these lenses and use a variety of lenses (accommodative, toric, monofocal and multifocal) to deliver the best possible vision for my patients' lifestyles.
Speak frankly about eyeglasses. My satisfaction results are lowest for basic lenses and highest for advanced technology lenses, despite the need for eyeglasses. IOLs aren't all about spectacle independence; they're about getting the best vision when patients want it most. Patients are satisfied when they use spectacles at the rate that you told them they'd be wearing them.
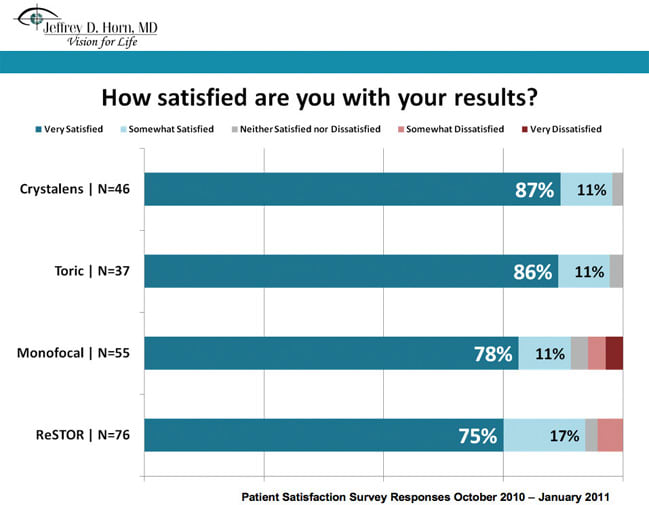
Figure 1. 87% of patients surveyed said they were very satisfied with the Crystalens.
I explain to patients that advanced technology lenses will give them the range of vision of a 45-year-old, and it will stay that way. It will return them to having excellent vision for distance and arm's length, but they'll need over-the-counter reading glasses for close work. If they choose basic lenses, they'll need stronger reading glasses for near and a second spectacle power for seeing at arm's length.
Ask patients what they want. To determine how patients' preferences and lifestyles will influence lens choice, I have them fill out a Vision Preferences Checklist. Patients answer questions that indicate situations in which they wouldn't mind wearing eyeglasses (near, mid-range or distance), based on examples of common activities. They rate the importance of good night vision; list hobbies; note how many hours per day they spend reading, driving, or on the computer; and place themselves on a personality scale from “easy-going” to “perfectionist.”
This gives me a good basis for choosing a lens, usually an advanced technology option. Patients understand that camera lens quality varies, and they also understand that IOL quality varies for their needs. Do they want to focus automatically on distance and mid-range objects? Then they want an advanced technology lens.
The Right Questions
Surveys tell us if we're succeeding in our goals by measuring patient satisfaction. Even if we achieve outcomes that we deem are average or above average, patient satisfaction is really our key indicator. If patients express dissatisfaction with their results, it's usually because the lens choice wasn't appropriate for that patient or because of misguided expectations.
I distribute satisfaction surveys to all of my lens replacement patients. Although surveys are voluntary, returned surveys generally match the proportions of lenses that I use (about 75% advanced technology and 25% basic).
When I reviewed the latest results, I evaluated 214 surveys returned between October 2010 and January 2011. Almost all patients were satisfied, but advanced technology lenses beat basic lenses. Of patients who received basic IOLs, 89% were very or somewhat satisfied with the surgical results. That number increased to 92% for Restor, 97% for toric lenses and 98% for Crystalens patients.
I found it interesting that the results showed no direct correlation between satisfaction and spectacle independence. When eyes are perfectly healthy, I recommend the Restor lens to help patients achieve spectacle independence. When patients can't use the Restor because of ocular pathology, I use the Crystalens. I explain that patients will wear eyeglasses more often for fine print but not for computer use. These are my most satisfied patients.
We have a high satisfaction rate across the board for all lens types, (ranging from 89% satisfaction for a basic IOL to 98% for Crystalens). But the satisfaction survey shows that although not all lenses work equally well, they work well when implanted in the correct eye of the right patient, and when we meet or exceed expectations. In other words, if I had implanted the basic lens in a percentage of eyes that received the Crystalens, or if I implanted a diffractive multifocal in some of the Crystalens recipients, my satisfaction rates would have been lower for the basic lens as well as the multifocal.
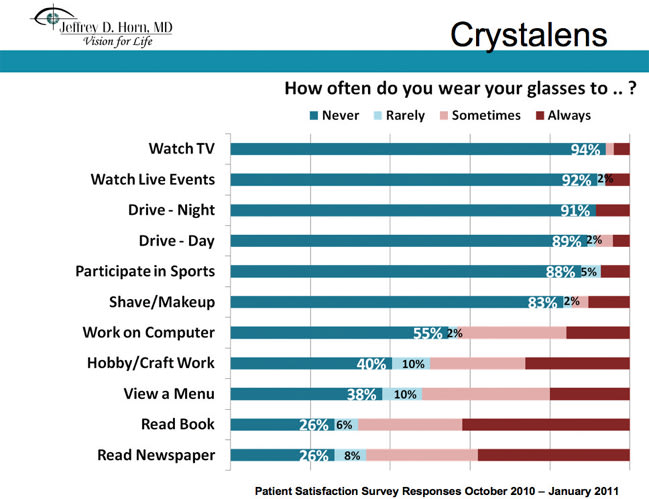
Figure 2. Patients expressed the highest level of satisfaction for Crystalens, compared to other IOLs, despite the fact that other lenses offered greater spectacle independence. As part of the education process, patients accepted this level of spectacle use before deciding on an IOL. Surgery met or exceeded their expectations, even with reading glasses.
A Full Toolkit
To give each patient the best lens, I need every lens available. With a variety of high-quality choices to serve a variety of patients, I carefully make a custom match to achieve the best outcomes and patient satisfaction. If you put the wrong lens in a patient or don't set expectations appropriately, patients won't be happy. But if you choose well and educate patients, they'll be happy almost every time—even if an advanced technology lens means they need eyeglasses some of the time.
| The Right Education |
|---|
| To ensure satisfaction, patient education begins when I inform a patient that he needs surgery for cataracts. My goal is to create a paradigm shift for this surgery by getting patients to focus on the solution, not the problem. I explain to them that just as knee replacement surgery isn't “arthritis surgery,” the procedure commonly referred to as “cataract surgery” is actually “lens replacement surgery.” I use a camera analogy in which the eye represents the camera and that camera has a lens. Over time, the lens becomes imperfect, which means that the photograph (vision) is imperfect, too. A camera repair shop will replace the lens, just as we'll swap the lens on the eye. The new, clear lens will likely stay clear forever. Rather than focusing on the cataract, I tell patients that the cataract itself isn't important. Once we identify it as a problem, what's important is the lens implant that we choose to replace it. We spend most of our time discussing that replacement, and I try to understand how the patient wants to see to enhance his or her lifestyle. When I survey all of my patients after cataract surgery, I ask them which lens they received. If I've done a good job in emphasizing the IOL and presenting the choices, then patients can name their lens. |
Dr. Horn is the owner of Vision for Life, where he performs LASIK surgery, laser vision surgery and cataract surgery in Nashville, Tenn. He was the first surgeon in Tennessee to perform laser cataract extraction and is a frequent speaker on ophthalmic surgeries.