This simple algorithm can help guide you to the proper code
By: RIVA LEE ASBELL
Ophthalmology Management May 1, 2010
E/M vs. Eye Codes: How to Choose? Part 3 of 3
Coding & Compliance, Done With Confidence
This simple algorithm can help guide you to the proper code
By Riva Lee Asbell
Since ophthalmology is the only specialty privileged with the option to choose between two sets of codes for outpatient services, for each encounter you must decide which is the best code to use. This should be based on three factors: compliance, medical necessity and financial optimization.
As we are nearing the end of the decision-making process, some distinguishing factors should be apparent. Eye codes are vague — there are no sharp divisions between history, examination and medical decision making. They are all lumped together, whereas the E/M codes are quite specific. I have found the E/M codes easier to defend under audit.
Eye code examination requirements vary among different Medicare contractors. You must have medical necessity for the service itself as well as each exam element you are performing. You cannot decide "I always bill 92014" twice a year. There must be medical necessity for the level of service in both sets of codes. The four elements of a comprehensive eye code exam and one element of an intermediate eye code exam are set by CPT dictate. You have no choice. Thus, there must be medical necessity for each element. In E/M codes, you have a choice of elements — it is a quantitative requirement. Any of the elements fulfill the numerical requirement as long as there is medical necessity.
Compliance means different things to us all, but in terms of Medicare coding and reimbursement, it means adhering to CMS regulations and making sure that your chart documentation supports the code and level of service that you have chosen. Medicare wants you to neither overcode nor undercode. Audits are conducted for both mistakes.
The following factors should guide you in making the final decision: compliance, local and national policies and, finally, financial optimization. There really is no problem in selecting a code that also is remuneratively rewarding.
Code Selection
For 2010, it has become imperative that you pay close attention to your coding. For many practitioners, especially subspecialists who were dependent on remuneration from the consultation codes, there will be a devastating reduction in revenue.
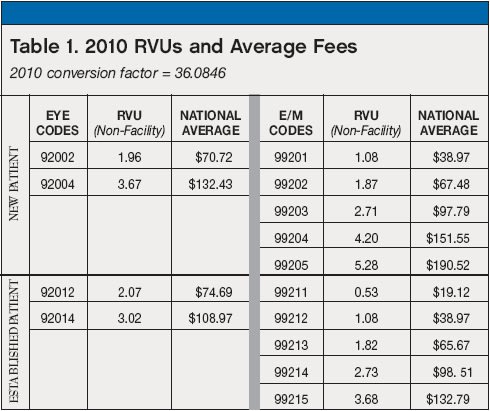
There are certain subspecialties, like oculoplastics, where the physicians would forego the dilated funduscopy examination on new patients/consultation. It is time to revisit and recalculate that. Without funduscopy the most you can bill would be an E/M level 3 new patient ($97.79), whereas with a dilated fundus exam you can bill a level 4 new patient ($151.55).
Table 1 is a chart showing the main codes available for coding office encounters in a non-facility setting. For 2010, there are overall gains compared to the latter half of 2009.
In reality, you probably will only be using five or so of the codes in everyday practice. Let's see how the algorithm works.
New Patients
Note: It might be worthwhile to review the first two parts of this article series before continuing. They can be found at www.ophthalmologymanagement.com, in the archives for the March 2010 and April 2010 issues.
If your level is 4 or higher, you should probably be using E/M codes. If your level is 3 or lower, you should probably be using eye codes unless you fail to initiate a diagnostic and treatment program at the comprehensive eye code level. Then you will have to drop to 99203.
Let's look at an example. A patient is examined with complaints of difficulty seeing out of the right eye. A comprehensive history is taken and a comprehensive exam is performed. It is determined that the patient has open angle glaucoma and dry macular degeneration. The adjective is moderate — so you would use CPT code 99204.
The next patient comes in with similar complaints, but has only an early cataract and receives a new prescription for glasses and instructions to return in six months. The adjective would be "low," so the level is 3. A comprehensive eye code (92004) is the better choice over the appropriate E/M code (99203).
Return office visits
There are a few key choices you need to make in these encounters.
92012 vs. 99213. For return office visits for conditions requiring more frequent exams, the choice is often between CPT codes 99213 and 92012. An error was made in the RVU calculation in 1998, and the erroneous calculation has been pretty much maintained. This has resulted in significantly higher reimbursement for code 92012 in 2010 — $9.02 more in 2010 on a national average. Given the choice, the eye code pays better than the E/M code and can be pretty much used in most instances.
Use 92014 for your follow-ups where medical necessity dictates a comprehensive examination, such as a return in one year for cataract follow-up. The code is not intended to be used for frequent follow-up visits for serious pathological conditions.
Use 99214 when following serious diseases as long as your medical decision-making is moderate and you have the medical necessity to perform nine of the elements. This code has been a target of OIG investigations and you should be confident of your coding skills and chart documentation when using it.
As a final note, I would like you to review the definition of a new patient. The CPT and Medicare's definition is one who has not received any professional services from the physician or another physician of the same specialty who belongs to the same group practice in a face-to-face encounter in three years. The definition of new patient incorporating "face-to-face" was revised several years ago.
In many established practices, that three-plus years goes by rather quickly and you are losing about 30% of potential reimbursement for the visit. For example, if you had been renewing glaucoma meds in a patient confined to a skilled nursing facility but had not actually examined the patient, if that patient were seen in the office it would be classified as a new patient encounter.
Conclusion
I hope that this series has provided you with a logical methodology for solving the dilemma when faced with choosing between E/M and Eye Codes. You should be mixing your use of the codes to maintain compliance while optimizing reimbursement at the same time. Good Luck! OM
Riva Lee Asbell can be contacted at www.rivaleeasbell.com, where you can order a CD of a new webinar entitled "History – The First Key Component," which was developed to accompany this article series.