







Keeping the Drug Pipeline Stocked
Will the next generation of anti-infectives be able to combat resistant strains of bacterial bugs?
BY LESLIE GOLDBERG, ASSOCIATE EDITOR
When the fourth-generation fluoroquinolones gatifloxacin 0.3% (Zymar from Allergan) and moxifloxacin 0.5% (Alcon's Vigamox) were introduced in 2003 to replace the previous generation of fluoroquinolones, there were concerns that overuse of these antibiotics could result in microbial resistance. But once their greater efficacy against bacterial conjunctivitis, blepharitis and keratitis was established, they were soon the most commonly prescribed antibiotics for treating corneal infections.
Unfortunately, emerging bacterial resistance to fourth-generation fluoroquinolones is now on the rise. The question is: will this increase be enough to alter doctors' treatment regimens or to motivate pharmaceutical companies to develop even newer generations of anti-infectives?
Doctors' Dilemma
"I think there is progressive evidence of resistance developing to fluoroquinolones, just as there is a progressive evidence of the spread of MRSA," says Herbert E. Kaufman, M.D., professor emeritus of ophthalmology, pharmacology and microbiology at Louisiana State University Medical School. Dr. Kaufman says that for some antibiotics like moxifloxacin, fungus has even been found growing in the antibiotic and that this is the problem of progressive resistance.
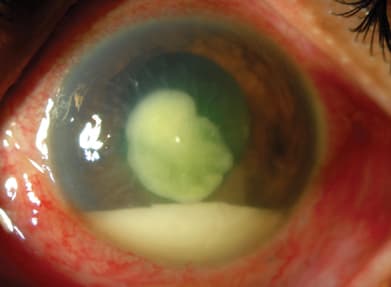
A patient with a severe central bacterial ulcer and a large hypopyon. Image courtesy of Christopher Rapuano, M.D.
"What concerns me is that it takes so many years to establish efficacy of safety and get a drug through the FDA. I'm bothered by the lack of drugs in the pipeline when there is a definite need for new antibiotics," says Dr. Kaufman.
He says that due to the nature of how antibiotics are used in ophthalmology, doctors don't have the time to wait and see what's causing an infection or to follow an antibiotic's resistance patterns. "If you start with a small cold or an infection, you can wait before going whole-hog. But if you have an infection in the eye, it is likely to be devastating within a day or two — that's the ophthalmologist's dilemma."
The Resistance
"MRSA infections are changing from a primarily hospital-acquired infection to a community-acquired disease process," said Vahid Feiz, M.D., of UC Davis Medical Center in Sacramento, at Cornea Day, preceding this year's ASCRS conference in Chicago.
Resistance to fluoroquinolones is on the rise, says Marguerite McDonald, M.D., F.A.C.S., in practice at Ophthalmic Consultants of Long Island in Lynbrook, N.Y. and clinical professor of ophthalmology at NYU School of Medicine. Dr. McDonald explains the that this increase is occurring for many reasons:
► The most common occurrence of resistance is through enzymatic inactivation or modification of the drug.
► Alteration of the target site is another reason. For fluoroquinolones, this involves mutations in DNA of target enzymes GyrA, GyrB, ParC and ParE subunits.
► Decreased uptake or increased efflux, such as the AcrAB efflux pump for fluoroquinolones, may also occur.
► Development of bypass pathways, such as the expression of alternate penicillin-binding protein, PBP2a, by MRSA is another reason.
► Lastly, acquisition of genetic material from other resistant organisms (conjugation, transduction, transformation)2 and acquisition of genetic material by mutation of DNA of ocular pathogen2,3 are possible.
Drugs in the Pipeline
"Unfortunately, germs continue to mutate and we need to stay on top of the trends in antibiotic resistance. The medications that we use will constantly be changing every several years to help us have choices that will continue to provide some effectiveness, but also safety for the eye," says David R. Hardten, M.D., F.A.C.S., a founding partner of Minnesota Eye Consultants.
"There are not a large number of antibiotics in the pipeline, and there are a lot of reasons for this," says Dr.McDonald. "Not every antibiotic is broad enough to meet all the criteria: having a broad enough spectrum, requiring at least two mutations for resistance, appropriate for application topically to the eye, etc. Also, the recession has impacted everything, including research and development."
Still, resistance increases the risk of treatment failure and it is essential to keep up the development of new drugs. Below is a list of drugs that doctors soon may have in their antibiotic armamentarium to combat these stronger more-resistant strain of bugs:
Bausch & Lomb's new fluoroquinolone besifloxacin ophthalmic suspension 0.6% is under development for the treatment of bacterial conjunctivitis. The drug includes InSite Vision's DuraSite, a biodegradable polymer that can maintain therapeutic doses of a drug on the ocular surface for up to 6 hours. Besifloxacin is indicated for t.i.d. administration and Bausch & Lomb aims to launch the drug later this year. Dr. McDonald says that besifloxacin is the first fluoroquinolone developed specifically for ophthalmic use, and the first ever used systemically.
RegeneRx is developing RGN-259, a Tβ4-based sterile eye drop, as a novel treatment for corneal healing. RGN-259 represents a new approach to corneal healing, as there is currently no pharmaceutical agent that has shown both tissue repair and anti-inflammation properties. Preclinical studies have identified cell migration, anti-apoptotic and antiinflammatory activities of Tβ4 in the cornea.4
"It is hard to predict when RGN-259 will go to market as it is in Phase 2 studies," says J.J. Finkelstein, president and CEO of RegeneRx. "It is not a drug used for bacterial infection. It is a drug that has been shown to be useful in corneal wound healing. So, we are not treating the organism but healing the corneal epithelium, so the cornea is intact and resists further damage." Mr. Finklestein says that there are no true wound-healing factors that are effective in the eye that he is aware of. "It will be used anywhere from a case of neurotrophic keratitis to corneal abrasions and surgeries where you want accelerated healing." The drug is a sterile eye drop to be used four times daily.
Lux Biosciences has completed three Phase 3 LUMINATE trials of the company's LX211 (Luveniq, voclosporin oral capsule) drug candidate for the treatment of uveitis. A poster presented at this year's ARVO by Michael Paterno et al. demonstrated a positive effect on ocular inflammation and a safety profile consistent with the expected use of LX211 in patients with bacterial conjunctivitis.
Lux notes that the integrated safety profile of 0.4 mg/kg b.i.d. LX211 in the LUMINATE trials suggests that it would be suitable for chronic use in this high medical-need indication.5
Inspire's AzaSite (azithromycin 1% ophthalmic solution) is not new as an indication for bacterial conjunctivitis, but Dr. McDonald says that it has a tremendous affinity for tissue. Inspire recently initiated phase 2 blepharitis trials evaluating the safety and efficacy of AzaSite vs. placebo at treatment durations of two and four weeks. "It is a completely new indication for the drug," says Dr. McDonald. "It is fundamentally different — it is not a fluoroquinolone. It is in a completely different family." It has been used for years for lung disease but was not available as an eye drop until formulated with DuraSite.
"It has an affinity for tissue and sticks to conjunctiva, cornea and the eyelids and is present in high concentrations in tears," she explains. Dr. McDonald says that AzaSite is not a replacement for fluoroquinolones and does not penetrate into the aqueous humor, but is a highly effective drug.
Positive Findings in Study Results
The Ocular Tracking Resistance in U.S. Today (TRUST) study evaluates in vitro antimicrobial susceptibility of Staphylococcus aureus, Streptococcus pneumoniae and Haemophilus influenzae to ciprofloxacin, gatifloxacin, levofloxacin, moxifloxacin, penicillin, azithromycin, tobramycin, trimethoprim, and polymyxin B in national samples of ocular isolates.
Antimicrobials tested represent six classes of drugs: fluoroquinolones (ciprofloxacin, gatifloxacin, levofloxacin, moxi floxacin), dihydrofolate reductase inhibitors (trimethoprim), macrolides (azithromycin), aminoglycosides (tobramycin), polypeptides (polymyxin B) and β-lactams (penicillin).
Study results from the TRUST 3 study were presented at ASCRS this past April. Below are some of the findings:
► With the exception of trimethoprim and tobramycin, less than one-third of MRSA strains are susceptible to ophthalmic antimicrobials.
► Susceptibility profiles remain virtually identical for the fluoroquinolones, regardless of methicillin phenotype.
► S. aureus is more susceptible to the fluoroquinolones than to macrolides.
► Fluoroquinolones continue to be the most consistently active agents against all pathogens tested in Ocular TRUST.
► Susceptibility patterns for 3-year period (2006 to 2008) are virtually identical for all fluoroquinolones and do not show a decline.6
There will always be a need for increasingly effective antibacterial drugs. And while some doctors may be hesitant to move on to the next generation right away, increased efficacy will surely mean eventual acceptance. OM
References
- Edmunds MW. Clinal Challenges of Methicillin-Resistant Staphylococcus aureus (MRSA). WebMD. Medscape. www.medscape.com/viewarticle/522947. Accessed June 12, 2008.
- Jensen HG, Felix C, and the In Vitro Antibiotic Testing Group. Cornea. 1998; 17:179-187.
- Mathews et al. Diag Microb Infect Dis. 2000;36:81-84.
- www.regenerx.com/wt/page/diabetic_vitrectomy. Accessed May 11, 2009.
- Lux Uveitis Drug Shows Positive Results. Retinal Physician. 2009;6:12
- Asbell P, M.D., F.A.C.S., M.B.A., Sahm D, Ph.D. and Shedden A., M.D., for the Ocular TRUST Study Group. Ocular TRUST 3: Ongoing Longitudinal Surveillance of Antimicrobial Susceptibility in Ocular Isolates. Powerpoint presentation accessed May 6, 2009.