







Moving Glaucoma Forward
It lacks the glamour of other subspecialties, but its rock-solid job security and the promise of innovations down the road offer a career path that practitioners young and old can follow.
BY LESLIE GOLDBERG, ASSOCIATE EDITOR

In the classic political exposé All The President's Men, two enterprising reporters hot on the trail of an exciting story are told to "follow the money." Anyone wondering why growth in the ranks of glaucoma specialists isn't keeping pace with the need for patient care can find the answer in much the same way.
Experts concede that there's more money, and perhaps more excitement, in other ophthalmic subspecialties right now, and that this can dissuade residents from pursuing a career in glaucoma. "I think today's residents are very much aware that they are ending up in debt — $50,0000 to $300,000 — which is unfortunate," says George L. Spaeth, M.D., director of glaucoma service at Wills Eye Hospital and Jefferson Medical College in Philadelphia. "Because of this debt, they feel they need to go into a field where they can make money. You can make more money in retina and cornea, in general, than you can in glaucoma." Given these economic realities, what can be done to lead new recruits to this sometimes overlooked but essential subspecialty? And what of the prospects for established glaucoma practitioners, whose financial fate is inextricably linked to their fickle patron Medicare? In this article, glaucoma specialists reveal why they wouldn't trade places with anyone — and why they feel ophthalmology residents are penny-wise but pound-foolish if they, too, follow the money.
Dollars and Sense
"All of us should read the essay we wrote to get into medical school," says glaucoma specialist Steve Mansberger, M.D., of Portland, OR. "None of us said anything about money." Rather, he says, the desire to be a part of innovations that improve lives and reduce risk of blindness were the motivations. But that doesn't mean the specialty is a losing proposition financially. "We all make a good living, and most of us are very satisfied with our careers," he says, likening it to the fable of the turtle and the hare. "Glaucoma specialists are slow and steady earners."
The field may lack a big-ticket item like premium IOLs or LASIK, he says, but then again, "every week we have patients coming in regardless of the economy." The recession-proof nature of glaucoma might seem pretty appealing right now to some corneal and cataract specialists who've seen fluctuations in their billings as patients scale back on out-of-pocket procedures. "There's a huge amount of job security in glaucoma," Dr. Mansberger says. "Every glaucoma specialist I know is swamped, and everyone is trying to hire people."
In an economy notorious for record-breaking unemployment figures, this stability can make the glaucoma field quite attractive to a resident or fellow looking for a viable career path. Indeed, Dr. Spaeth says his institution has received better applicants for its fellowship program this year than they've ever had in the history of the application process. He says the institution had 25 superb applicants for three positions.
Dr. Spaeth realizes that he is in a privileged position where he has fewer concerns about expenses, but acknowledges the challenges to young ophthalmologists. "There's a lot of pressure put on physicians, but the ultimate reward of medicine is taking care of people who are sick and challenge you." While glaucoma patients can be difficult to treat, these cases can also be more rewarding. "The wonderful part of medicine is trying to figure out how you can help someone, because you can always help someone no matter how desperate the situation." Dr. Mansberger, who among his other responsibilities serves as director of glaucoma service at Portland's VA hospital, echoes that sentiment.
Glaucoma Practice: Under Pressure
How do you enhance the appeal of glaucoma as a specialty so that residents are more attracted to it? Andrew Rabinowitz, M.D., a glaucoma specialist based in Phoenix, says that because glaucoma is a chronic disease, its practitioners also have to serve as the patient's advisor and confidant. He thinks that some residents may be uncomfortable in this role, although he considers it a rewarding aspect of the physician-patient relationship.
Because of the chronic nature of the disease, Dr. Rabinowitz believes that glaucoma practice is better suited to empathetic physicians who welcome long-term relationships with patients. "Residents are seeing a dichotomy in the clinic. With retina, they see doctors performing surgeries or giving shots of Avastin and the patient getting better. Similarly, cataract and refractive surgeons provide instant gratification to their patients. Yet in glaucoma, residents don't see a way to offer immediate results," says Dr. Rabinowitz. In fact, most glaucoma procedures expose the patient to at least some risk that vision will worsen following surgery.
"In the past, I was able to tell patients that possible loss of vision was a tradeoff for preserving their vision for the rest of their lives, and they understood this," says Dr. Rabinowitz. "But now, society equates eye surgery with visual improvement. Patients are socialized by what they see in the media. Even though we say that we are unable to deliver this outcome, they have a difficult time getting their mind around it." Patients have become risk averse and are less likely to accept the risk of surgery early on. "From the time I started practicing 14 years ago, the number of glaucoma surgeries has declined nearly 75%," he says. "A great deal of this decline has to with the availability of better medications, but a change in the whole patient-doctor dynamic has occurred as well."
Dr. Rabinowitz explains that in glaucoma, because treatments do not improve vision, it is extremely important to build relationships with your patients and to discuss expectations. "There has been a breach of doctor-patient confidence," says Dr. Rabinowitz. He says that as a physician, he notices that most doctors practicing in other fields of medicine are so busy moving through their day that they don't have five minutes to spend with their patients. "Patients go to doctor after doctor with these chronic illnesses and are so disenchanted with the system that they have lost faith in the doctor."
Better Options, Brighter Future
Surgical techniques with improved safety profiles may rekindle enthusiasm for interventional approaches and, by extension, for the glaucoma field as a whole. "The issue with glaucoma surgery has not been its effectiveness, but rather the long-term complications and the intensity of care required after surgery," says Dr. Cantor. "Many of the basic concepts of glaucoma surgery have not changed dramatically in the last few decades and I think that's where a lot of the perception has been that there is not much to do surgically," he says.
On the other hand, he thinks that the glaucoma community is considering glaucoma surgery earlier on in their patients and being more aggressive. "The options for medical therapy have certainly expanded," says Dr. Cantor, "but many glaucoma patients cannot be controlled with medications and require laser and surgical management. The problem is, we often delay surgical management because of concerns over some of the issues surrounding surgery."
Dr. Cantor thinks that if there were a more controlled surgical approach to glaucoma and a safer and more acceptable procedure available, surgery could be considered as a primary therapy. He thinks this is likely to change in the next five years, as there is a lot of interest in new surgical approaches and devices. "Most of us are concerned that many of the filtering blebs we create are sort of ticking time-bombs, that eventually there is a pretty substantial risk of developing problems," says Dr. Cantor. "While the current surgeries work very well at keeping the pressure down and are effective in preventing glaucomatous damage, it's the safety of the surgery, not the efficacy, that has been our problem."
In addition to innovations on the surgical front, novel drug delivery methods have the potential to alter the equation as well. "We have many wonderful medicines at our disposal right now," says Dr. Mansberger, and exciting research is likely to yield notable improvements. Sustained-release injectable drugs, he says, are "low-hanging fruit" that will add to a glaucoma specialist's options within the next five years. Anti-VEGF therapies transformed retina in recent years, and glaucoma is capable of breakthroughs of that magnitude as well, he says.
Different Paths, Same Destination
"While glaucoma will still be a lifelong disease, the development of new surgeries for glaucoma will provide physicians with more satisfaction," says Dr. Cantor. In the meantime, Dr. Cantor recommends that doctors prioritize their time where it really matters: with patients. "The key to maximizing patient-physician time is not to perform inefficient tasks like writing out prescriptions. Talk to your patient about ways to improve their compliance. Quality time can still be spent with your patient, even with the current constraints."
Dr. Cantor believes that across the entire spectrum of healthcare, teams and collaboration are going to become more important, especially when looking at some of the reforms in healthcare financing. "This is going to necessitate, if not demand, greater use of physician extenders and allied health professionals," says Dr. Cantor. "For example, retina specialists see so much diabetes, they can't possibly keep up with the demand of screening every diabetic every year. There aren't even enough ophthalmologists to do it. I think we will see an increase in collaborative teams."
How this will work needs to be determined locally, he says. For some telemedicine may work, for others co-management. Still others may build or join multispecialty group practices. "There are lots of ways to establish healthcare systems to provide care where there is not a system in place now to serve the public well," says Dr. Cantor.
Any efficiency gains that free up more of the glaucoma specialist's time to spend with patients will improve patient care and allow the practice to see more patients, steadily increasing billings. But sometimes the easiest way to bolster the financial aspect of glaucoma practice is simply to be more vigilant in how your billing and coding is done, frequently reevaluating your approach and looking for missed opportunities (see "Increasing Revenue in the Glaucoma Practice" below).
| Increasing Revenue in the Glaucoma Practice |
|---|
The category of codes known as Prolonged Services are not usually used in ophthalmology, but have great use in the glaucoma practice. These codes, revised in CPT 2009, can be used for those patients who remain in the office for a prolonged period and need intensive care such as when a patient with acute glaucoma presents. There are two sets of codes in CPT: One for services with face-to-face contact and the other without. In the glaucoma practice we are concerned with when a physician provides prolonged service involving direct (face-to-face) patient contact that is beyond the usual service in either the inpatient or outpatient setting. This service is reported in addition to other physician services, including evaluation and management services at any level. An appropriate code should be selected for procedures performed in the care of the patient during this period. Here are the codes: +99354: Prolonged physician service in the office or other outpatient setting requiring direct (face-to-face) patient contact beyond the usual service acute asthmatic patient in an outpatient; first hour (List separately in addition to code for office or other outpatient Evaluation and Management service) +99355: each additional 30 minutes (List separately in addition to code for prolonged physician service Here is the table to make the calculations: 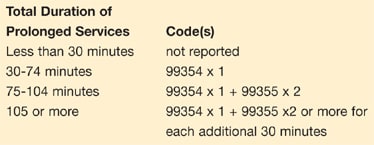
Here are some tips to help you: • Time counted must be face-to-face time with the physician and not auxiliary personnel • Time counted is for the total duration of face-to-face time that the physician spends with the patient, even if the time is not continuous • The codes reported must be the time equivalent of the E&M code plus an additional 30 minutes before you begin your calculations. Each code's typical time allotment is noted in its CPT description; for example, the typical time for a level 4 consultation is 60 minutes • There are separate consultation codes for inpatient and outpatient services • Do not use for counseling or coordination of care • The national average (non facility) for the outpatient codes for 2009 are: +99354 — $ 91.97 +99355 — $ 90.88 • CPT uses the symbol + before a code to designate the code as an add-on code. Add-on codes do not take modifier -51 and pay at 100% of the allowable for that code • Be sure to document your face-to-face time precisely Here is an example to help you: Patient is seen for evaluation of painful red eye after being examined by an outside physician. Patient has acute glaucoma and spends the day. Documented physician face-to-face time is 3 hours, 15 minutes. Total duration of prolonged services is 105 minutes (Consult = 60 minutes CPT typical time + 30 mandatory waiting minutes) The Math: 195 minutes (face-to-face time) minus 90 minutes (from the consult + 30 minutes mandated non billable time) = 105 minutes. Code and bill: 99244 Level 4 consult ($184.34) 99354 × 1 and 99355 × 2 ($91.97 + $90.88 × 2 = $295.59) Thus, on a national average, we have gained an extra $273.73 in addition to the consult. |
Frost/Nixon
Glaucoma and aging are as inseparable as Woodward and Bernstein once were, and the aging of the baby boomers makes it an inevitability that demand for glaucoma services will continue to increase. "There is a lot of opportunity, from a business aspect, to get into this growing market," says Dr. Cantor. "We not only have a growing aging population, we also have a situation where half of the people who have glaucoma don't even know it. Even today, if we could just get more of these people in to our offices — through education, promotion and screening — there is a potential for doubling the people who need glaucoma services now."
Dr. Rabinowitz says that while retina has advanced 50 years technically over the past 10 years, glaucoma hasn't moved at all — there are simply safer meds. "Until there is surgical advancement in glaucoma, it will be difficult to compete with other subspecialties. This is not the place for personalities looking for instant gratification but it is a wonderful, passionate field," he concludes.
"Two roads diverged in a wood," Robert Frost wrote, "and I took the one less traveled by — and it has made all the difference." Many glaucoma specialists seem to share that sentiment. OM