







OCULAR SURFACE DISEASE SERIES: CASE STUDY #5
Without Rhyme or Season
Florida's climate puts a new spin on seasonal allergic conjunctivitis — and sends one patient into perennial discomfort.
By Charles B. Slonim, M.D., F.A.C.S.

Approximately 50 million Americans suffer from allergies. Among them, about 75% present with allergic rhinitis, which often is associated with ocular symptoms.1
Far from being the worst problem our patients face, seasonal allergic conjunctivitis (SAC) is nonetheless a common source of inflammation and discomfort. SAC gets patients out of their contact lenses, and sometimes sends patients out of their minds from the infuriating symptoms. What's more, the itching, redness and inflammation can delay elective surgery or complicate recovery.
I see a great deal of SAC in my Florida practice as various plants and trees flower throughout the year. Ocular allergy is ever-present, but it's also relatively simple to diagnose, and newer medications help us quiet acute episodes and manage the disease.
Key signs point to allergy
Like other types of conjunctivitis, SAC affects the ocular surface. When the seasonal allergen emerges outdoors, a patient may go from having comfortable, quiet eyes to experiencing acute, moderate or mild symptoms. In contrast, patients with PAC typically have mild-to-moderate symptoms year-round, sometimes with occasional acute episodes.
Patients with SAC often have a family history of allergies, asthma or eczema. They typically present with other allergy symptoms, such as a runny nose and sneezing. We also look for these telling ocular signs and symptoms, which occur bilaterally:
■ Itching that causes patients to rub their eyes
■ Swelling of the eyelids and conjunctiva
■ Papillae on the palpebral conjunctiva
■ Redness
■ Watering
■ Burning
■ Photophobia.
Although itching almost always points to allergy, these symptoms can occur in patients with other types of conjunctivitis or even dry eyes. Certain physical findings and diagnostic signs may help rule out the alternative "red eye" diagnoses:
■ Purulent discharge, as well as symptoms that started or continue to exist in only one eye or both eyes, indicate that a possible bacterial infection is causing the conjunctivitis.
■ A preauricular lymph node or the presence of corneal infiltrates may signify conjunctivitis of a viral origin.
■ Staining indicates the presence of keratitis, suggesting that the patient may have moderate or serious dry eye.
Patient exhausts OTC options
"It's driving me crazy!" a frustrated patient told me. "I feel like I have to rub my eyes to stop the itching, but I'm only comfortable for a few minutes before the itching starts again." The 43-year-old woman came to my office complaining of itching, watering and occasional burning in both eyes.
She knew she had allergies because her eyes weren't the only problem. She was sneezing and had a runny nose, too. Her symptoms began about a week before as she was doing yard work. As the day wore on, she started rubbing her eyes and the itching became worse.
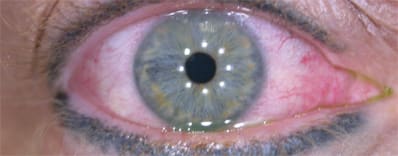
Seasonal allergic conjunctivitis can be identified by these telling ocular signs and symptoms: itching, swelling of the eyelids and conjunctiva, papillae on the palpebral conjunctiva, redness, watering, burning and photophobia.
The patient then bought some over-the-counter allergy medications. She was taking loratadine and pseudoephedrine (Claritin D), which gave her some relief from the sneezing and runny nose, but didn't help her ocular symptoms.
She tried over-the-counter antiallergy eye drops, including pheniramine maleate 0.3% with naphazoline hydrochloride 0.025% (Visine Advance Allergy) and naphazoline hydrochloride with antazoline phosphate (Vasocon-A), but these products made only a small, temporary dent in her acute symptoms.
Exam confirms diagnosis
I suspected an ocular allergy (ie, SAC) in this case and proceeded to the exam. The symptoms had no effect on the patient's visual acuity, which was 20/20 uncorrected. The slit lamp showed that her lid margins were fine, but there was a mild papillary reaction on the lower palpebral conjunctiva. The bulbar conjunctiva had +2 edema.
The patient was producing a clear, watery tear and the absence of pus made infection unlikely. I ruled out a viral component due to the absence of preauricular lymphadenopathy. The cornea also was clear. The patient had no fluorescein or lissamine green staining, which ruled out a corneal and/or conjunctival epitheliopathy (eg, chronic dry eye problem). Finally, the patient's anterior chamber was quiet with no cells or flare. These results, combined with the obvious presence of systemic allergy, meant that SAC was the most likely diagnosis for this patient.
Meeting acute and chronic needs
The patient had a moderate allergic reaction, and the symptoms were making her miserable. To reduce the conjunctival edema, I prescribed loteprednol etabonate 0.2% (Alrex®) right away, every couple hours for 2 days*, followed by four times a day until her symptoms changed. When she returned after 1 week, her eyes were much quieter and more comfortable.
Because something's always blooming in Florida, this patient returned 2 months later to complain that she'd been experiencing mild symptoms for a few weeks. I advised her to stop using OTC drops and prescribed azelastine hydrochloride 0.05% (Optivar), an antihistamine and mast cell stabilizer drop, twice a day whenever her allergies acted up. I also told her that if she had another exacerbation or acute episode, she should return for another round of loteprednol along with azelastine.
For patients with PAC, this combination of chronic and acute treatments is a good long-term approach. However, if the allergic response to year-round pollens is severe, patients may require a long-term topical steroid. The safety profile of loteprednol makes me comfortable prescribing it long term.
Dr. Slonim is clinical professor of ophthalmology at the University of South Florida College of Medicine in Tampa. He is also in private practice in Tampa.
| Case Study: Classic SAC |
| Sex: Female Age: 43 Signs and symptoms: ■ Itching, watering and occasional burning in both eyes ■ Sneezing and a runny nose Exam: ■ Visual acuity 20/20 uncorrected ■ Mild papillary reaction on lower palpebra ■ +2 edema on bulbar conjunctiva ■ Clear, watery tear ■ No preauricular lymph node swelling ■ No fluorescein or lissamine green staining ■ Quiet anterior chamber History: ■ Symptoms started while doing yard work ■ OTC oral allergy meds and allergy eye drops failed Diagnosis: Moderate SAC Treatments: ■ Loteprednol etabonate 0.2% (Alrex) every few hours for 2 days, then four times a day until her symptoms changed Outcome: ■ Loteprednol etabonate 0.2% eliminated the redness and swelling within 1 week. The patient later showed signs of PAC, and she began chronic use of a mast cell stabilizer, which was augmented with loteprednol etabonate 0.2% whenever another acute episode occurred. |
Reference:
1.Asthma and Allergy Foundation of America, "Allergy Facts and Figures." (www.aafa.org/display.cfm?id=9&sub=30) Last accessed 8/17/07.
Alrex is a registered trademark of Bausch & Lomb, Inc. Other brands listed are the trademarks of their respective owners.
Indication
ALREX® Ophthalmic Suspension is indicated for the temporary relief of the signs and symptoms of seasonal allergic conjunctivitis.
Important Safety Information
As with other ophthalmic corticosteroids, ALREX is contraindicated in most viral diseases of the cornea and conjunctiva, and in mycobacterial and fungal diseases of the eye. Prolonged use of corticosteroids may result in secondary glaucoma, cataract formation, and secondary ocular infections following suppression of the host immune response and/or perforation of the globe. The most common adverse events in patients treated with ALREX were abnormal vision, blurring, burning, chemosis, discharge, dry eyes, epiphora, foreign body sensation, itching, and photophobia. Non-ocular adverse reactions include headache, rhinitis, and pharyngitis.
*This is the dosage prescribed by the doctor, but the approved, recommended dosage is 1 drop instilled into the affected eye(s) 4 times daily.
For complete prescribing information, please see package insert available at: http://www.bausch.com/en_US/ecp/pharma/product/alrex_ecp.aspx