







VISANTE OCT: ANTERIOR SEGMENT IMAGING AND BIOMETRY
Applying OCT to Corneal Refractive Surgery
Unprecedented detail provides improved safety and accuracy.
By Jack T. Holladay, M.D., M.S.E.E., F.A.C.S.
The Visante OCT system for anterior-segment imaging and biometry assists refractive surgeons in many ways. For corneal laser refractive surgery, it aids in patient selection and treatment planning.
■ Surgeons can plan the procedure to ensure preservation of enough stromal tissue to prevent ectasia.
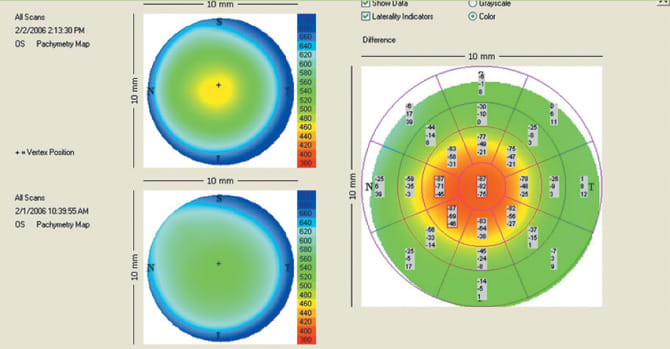
■ Pachymetry maps confirm adequate corneal thickness and detect corneal thickness irregularity. The maps provide low, high and average corneal thicknesses for multiple locations. The center of the maps is at the center of the thinnest part of the cornea, which is the geometric or anatomic center.
■ High-resolution image analysis evaluates corneal appearance for the presence of pathological or unusual morphology.
■ Anterior-segment image analysis helps surgeons determine whether phakic IOL implantation or another refractive procedure may be a better solution for a patient.
The Visante provides an unprecedented level of detail for the corneal refractive surgeon. We can think of that detail as a microscopic view of a forest. Topography and other technologies based on reflected light provide only a macroscopic view, the umbrella of leaves at the top of the forest. But OCT customized for the anterior segment allows us to actually look at the leaves. As a result, we are able to see things we were unable to see before.
The Visante OCT system also allows the corneal refractive surgeon to better assess procedure outcomes. It is the first noncontact instrument to image, measure and document corneal flap thickness and residual stromal thickness following LASIK. Its capabilities improve several aspects of postoperative care.
■ Surgeons can evaluate and document the thickness and regularity of flaps created by mechanical microkeratome or femtosecond laser. This is done without relying on preoperative calculations, lifting the flap, measuring the stromal bed or calculating the difference, all of which induce inflammation and ultimately thwart reliable measurements.
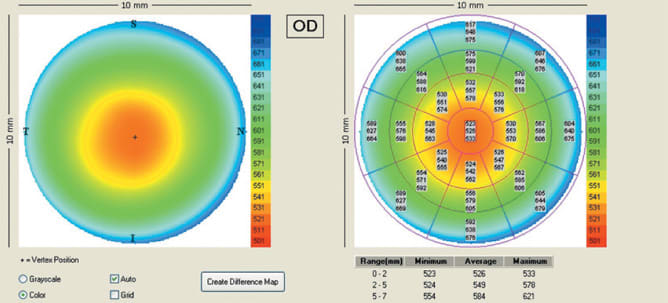
A Visante OCT pachymetry map indicates a normal corneal thickness pattern (circular) in the right eye of this patient.
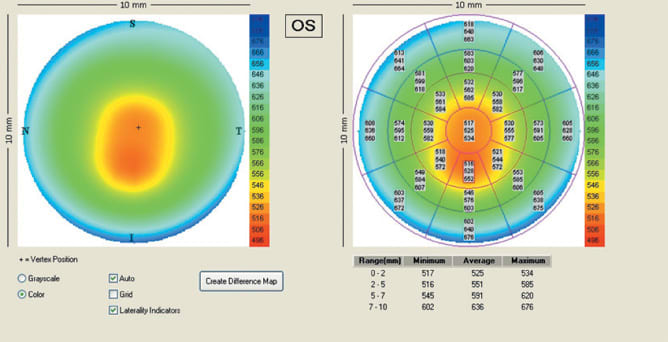
The pachymetry map of the left eye of the same patient reveals abnormal (oval or elongated) corneal thinning inferiorly. The thinning is illustrated by the qualitative map and the quantitative values.

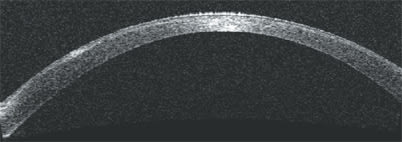
The area of corneal thinning indicated by the Visante OCT pachymetry map is also visible on the anterior-segment scan.
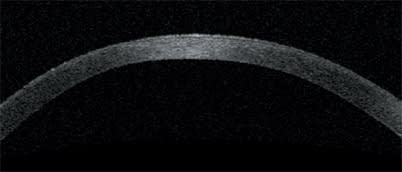
The high-resolution corneal scan provides anatomic validation of the thinning indicated by the pachymetry map and the anterior-segment scan.
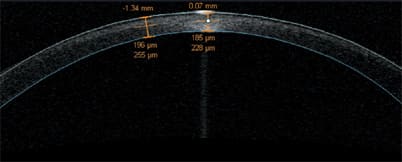
A high-resolution corneal scan and analysis confirms a residual stromal bed thickness of 228 μm, a contraindication for a LASIK enhancement procedure.
The Visante OCT reveals elevation caused by epithelial ingrowth (left mid peripheral area) following LASIK. Monitoring ingrowth is crucial in order to avoid thinning and buttonholing of the flap that would require its removal.
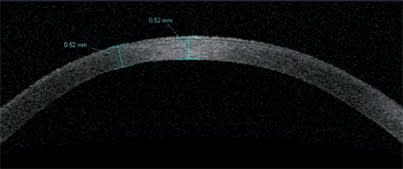
Applying the measurement tool to the high-resolution corneal scan of the left eye serves as further confirmation that LASIK is contraindicated for this patient.
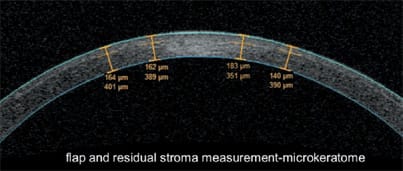
This slide shows Visante OCT measurements of flap and stromal thickness following LASIK. It's clear that the thickness of this flap is not uniform. The measured thickness values range from 140 μm to 183 μm.
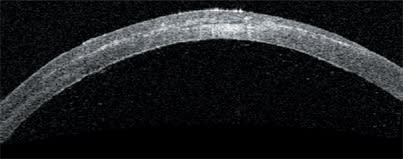
This high-resolution corneal scan shows fluid under a LASIK flap (centrally), the result of an inflammatory response.
This Visante OCT-generated post-LASIK ablation profile with pachymetry difference maps documents thickness, width and centration.
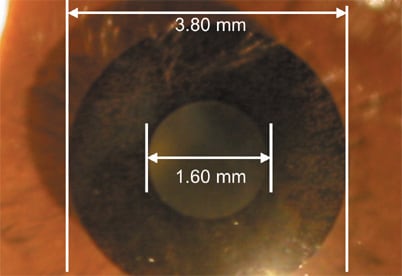
This is an external view of an experimental intracorneal implant (AcuFocus inlay) for the correction of presbyopia.
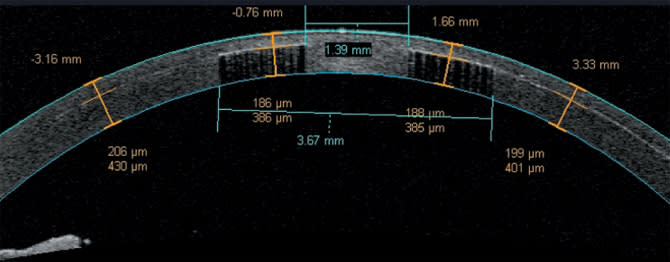
The Visante OCT shows the flap made for implantation of the intracorneal refractive implant. The surgeon can visualize the implant's edge and the light coming through its fenestrations.
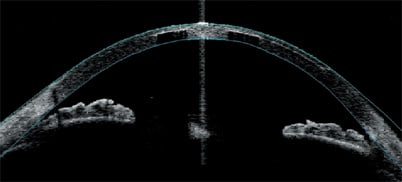
The anterior-segment profile includes the iris and the angle for precise location of the intracorneal implant.
Documenting the consistency of flap depth and the standard deviation of microkeratomes is becoming even more important as we move toward sub-Bowman's keratomileusis (SBK), which involves flaps as thin as 90 μm.
■ Awareness of post-op corneal morphology helps us prevent and manage flap-related complications.
■ Residual stromal thickness is quantified to confirm the feasibility of future enhancement procedures. It is no longer necessary to estimate the thickness of the stromal bed by assuming a typical flap thickness.
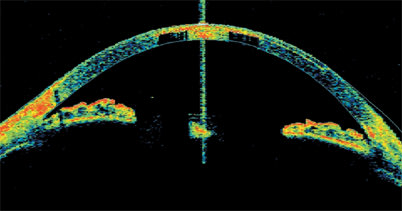
Depicting density, the color version of the anterior-segment scan shows lower amplitudes as blue colors and larger amplitudes as red colors.
The color version of the high-resolution corneal scan shows the useful light coming through the implant's aperture and the scattered light coming through the implant's fenestrations.
■ Post-op pachymetry difference maps document the laser ablation profile with respect to thickness, width and centration.
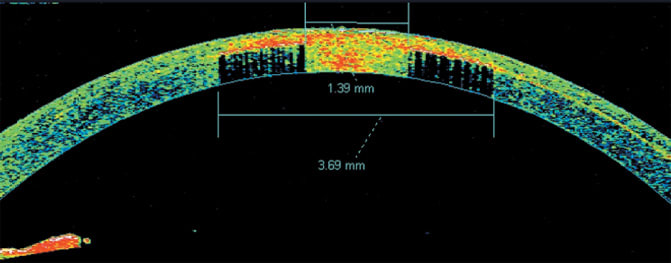
The Visante OCT also is proving to be useful in association with intracorneal refractive implants. The OCT images on this page depict an ultra-thin intracorneal implant currently being evaluated in patients for the correction of presbyopia (AcuFocus Inc.). Based on small-aperture optics, an optimized pinhole, the implant is 3.80 mm in diameter and has a 1.60-mm aperture.
The Visante OCT's high-resolution corneal scan and anterior-segment scan pinpoint the location of the implant and allow measurement of its diameter and thickness.
As this implant was being developed, the Visante OCT allowed documentation of the amount of scattered light coming through the implant's fenestrations. This allowed researchers to determine what level of light passing through caused glare and reduced contrast and what level did not affect patients' contrast sensitivity. OM