







A Guide to Successful DSAEK Technique
Q & A with two leading DSAEK surgeons.
Following is a discussion with Mark S. Gorovoy, M.D., and Massimo Busin, M.D., on their methods of performing Descemet’s-stripping automated endothelial keratoplasty (DSAEK) and issues they perceive in using pre-cut tissue:
Q: What is your experience with DSAEK?
Dr. Busin: I have performed about 100 DSAEK procedures to date. The improvement in refractive results and the increased safety of a closed-system procedure compared to an "open sky" penetrating keratoplasty (PK) make DSAEK a very important advance.
Dr. Gorovoy: DSAEK is indicated for patients with endothelial failure. Even dense edema is not a contraindication. I do think it is best to select patients who are pseudophakic, with a posterior-chamber lens.
I have now performed more than 400 DSAEK procedures and have personally instructed about 70 surgeons in the technique in my OR. This procedure has revolutionized corneal transplantation for endothelial dysfunction. Before, with penetrating keratoplasty (PK), the refractive results were very unpredictable and could take a year or more to stabilize. By contrast, the vast majority of DSAEK patients are seeing 20/40 within 6 weeks after surgery. The results are so superior that I no longer perform PK and would not recommend it for patients with endothelial disease.
Q: What is your current DSAEK technique?
Dr. Gorovoy: The procedure has been evolving, particularly in terms of the wound. I perform DSAEK under topical anesthesia. First, I measure the patient’s corneal diameter to determine what size tissue I want to insert. In about 75% of cases, I will use a 9-mm button, although I sometimes use an 8.75-mm or even smaller button on rare occasions. Using the Moria DSAEK system, the donor cornea is mounted on an artificial anterior chamber. I use the Moria CB microkeratome (Moria, Antony, France) with a 300-μm head to cut an anterior lamellar cap, and then punch the appropriate size button from the posterior portion of the cornea. I do not mark the tissue.

Figure 1. Dr. Gorovoy: The folded donor tissue can be inserted into the anterior chamber with a modified Gossey forceps.
Once I am satisfied with the donor button, I go back to the patient and make my clear corneal incision. The standard incision is 5 mm. Recently, I have been making smaller 3.2-mm incisions, but the rate of endothelial loss with this approach has yet to be fully validated. I also make several 1-mm paracentesis wounds in the limbus.
Through the paracentesis wounds, I introduce an irrigating stripper and strip Descemet’s membrane circumferentially, just inside the trephine mark. Next, I use a phacoemulsification irrigation & aspiration (I&A) tip to aspirate the membrane. Then I make three full-thickness venting stab incisions midperipherally, as described by Dr. (Francis W.) Price.
I make a 60/40 fold in the donor cornea with a small amount of Healon (Advanced Medical Optics, Santa Ana, Calif.) on the endothelial side in the center. Using a modified Goosey forceps I insert the folded tissue through the 3.2-mm keratome incision (Figure 1). To unfold it, I go back in with the I&A unit and aspirate the posterior fold. Once it has fully unfolded, I shallow the chamber slightly, making sure the tissue is well centered, and then insert a 100% air bubble in the anterior chamber. Finally, I drain the venting incisions. The eye is left high/normal-tensive with the air bubble and no sutures.
The patient is dilated and spends the next hour lying supine in the recovery room. Before discharging patients, I examine them at the slit lamp and expel some of the air from the anterior chamber until the air bubble clears the bottom of the pupil. This eliminates the risk of pupillary block. We start the patient on a fluoroquinolone antibiotic and prednisone q.i.d. and place a shield on the eye until the next day.
Dr. Busin: My technique differs substantially. I use a blunt cannula with an attached air syringe to break and strip Descemet’s membrane and remove it, usually in a single piece. Preparation of the donor cornea is as Dr. Gorovoy described, although I feel it is particularly important to mark the tissue, for two reasons. First, I mark on the posterior lamella the outer limit of the area from which the anterior stroma has been excised, in order to avoid punching through its outer edge. Even more importantly, a central mark (I usually use the letter "F") on the stromal side of the donor lamella allows the surgeon to distinguish it from the endothelial side after the graft has been inserted into the anterior chamber.
I also have a different method for inserting it that I find to be simpler and gentler to the endothelium. Instead of making a taco fold, I place the tissue on a specially designed glide (recently introduced by Moria as the Busin Glide Spatula and Forceps) with the endothelium up and drag it into the anterior chamber by means of a crocodile vitreous forceps inserted through a paracentesis performed opposite to the surgical wound (Figure 2). While sliding into the glide, the tissue folds onto itself on both sides but the endothelium remains untouched. As the two sidefolds are approximately 20% of the entire width, unfolding is also much less problematic, even in a shallow anterior chamber. To obtain maximum adhesion, it is very important to ensure that no viscoelastic remains between the donor and recipient tissue. I avoid pupillary block by performing a surgical peripheral iridectomy prior to inserting the graft.
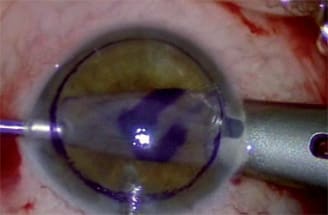
Figure 2. Dr. Busin: Alternatively, the donor tissue may be grasped with a forceps inserted through a temporal paracentesis incision and pulled into the anterior chamber from the Busin glide positioned at the entrance of a nasal clear-corneal tunnel.
Q: What is your dislocation rate?
Dr. Busin: Up to now, I’ve had four cases in which it was necessary to go back postoperatively and place a second air bubble, so my dislocation rate is 4%.
Dr. Gorovoy: Dislocation rates have been dropping with improvements in the procedure. In my last 100 cases, 9% dislocated. However, I would say the rate is only about 4% in eyes with "normal" anterior segments — that is, eyes in which there is no communication between the anterior and posterior chamber. Dislocation is more likely in eyes with shunts or previous vitrectomy. I think it is realistic to aim for a dislocation rate of 5% or lower for all comers.
Q: Some surgeons have been using tissue dissected in advance by eye banks for DSAEK. What are the potential clinical advantages or disadvantages of using pre-cut tissue?
Dr. Busin: The major disadvantage of pre-cut tissue is that it is associated with a higher rate of graft dislocations than tissue cut by the surgeon. Jayne Weiss, M.D., of the Kresge Eye Institute, has analyzed mid-2006 survey data from the North Carolina Eye Bank on the outcome of its pre-cut tissue grafts and found dislocation rates of 34% and graft failure rates of 23%. While these rates may be due in part to the learning curve of inexperienced surgeons in the survey, they are unacceptably high. By comparison, I had two primary graft failures in my first 10 cases, and none since then.
Additionally, pre-cut tissue is typically thicker than tissue you cut yourself. In some cases, it may be up to 20% thicker and thus difficult to handle. Furthermore, if you do not cut your own tissue, you do not have the opportunity to mark it, so it can be quite difficult to orient correctly in the eye. The only advantage of pre-cut tissue is that it provides surgeons the opportunity to perform DSAEK rather than PK if Moria equipment is not available.
Dr. Gorovoy: The primary graft failure rate should be about 1% — certainly not close to one-quarter of the cases. However, I think we need to see data from the same surgeons comparing pre-cut tissue vs. their own dissections to know whether the tissue itself is really having an impact on failure rates. We typically think of graft failures as surgeon-induced.
I am more concerned that swelling of the pre-cut donor tissue may contribute to dislocation. One of the mysteries of DSAEK is that we don’t really know what causes the tissue to stick. It has something to do with the stromal-fibril interaction and intracellular adhesions. If the cells are swollen and distorted, they might become less adherent, although we don’t fully understand this mechanism.
My daughter, Stacey Gorovoy, M.D., recently presented a paper at The Cornea Society and Eye Bank Association of America’s Federated Scientific Session in which she analyzed a series of 148 of my DSAEK cases. She found that donor tissue used in these 148 cases and preserved in Optisol (Chiron Ophthalmics, Irvine, Calif.) prior to dissection for longer than 3 days was twice as likely to detach. Moreover, tissue preserved for more than 5 days was three times as likely to detach. This is believed to be related to increased swelling the longer the tissue is in the media. Pre-cut tissue is going to swell even more because the stroma is directly bathed in the media. I spoke with one surgeon who told me that almost all of the cases he had performed with pre-cut tissue had dislocated. It turned out that the surgeon was waiting about 48 hours after the tissue was cut before using it, which may account for his problems with dislocation.
Dr. Busin: Overly swollen tissue is undesirable for several reasons. The first is the risk of dislocation that we’ve been discussing. But, in addition, a thick, swollen donor button is more difficult to handle and insert and harder to manipulate once inside the eye. Overmanipulation of the tissue may increase endothelial cell loss and could even lead to graft failure. If there is a lot of edema, it will also take longer for the cornea to clear, delaying visual rehabilitation.
Q: What do you feel is an acceptable rate of endothelial cell loss for DSAEK?
Dr. Busin: Better technique and more experience, particularly with insertion of the donor button, can protect the endothelium. I went from an average of nearly 50% endothelial cell loss at 6 months when I began performing DSAEK to 20%-30%, which is comparable to PK. I think we need to achieve cell loss rates that are comparable to the current standard procedure, PK.
Dr. Gorovoy: We are now conducting studies on the endothelial cell loss after DSAEK. I am optimistic that the endothelial results will be similar to PK, but even if they are not, the results are so superior to PK that DSAEK would still be the procedure of choice.
Q: Are you concerned at all about the impact of pre-cut tissue on the tissue supply?
Dr. Busin: I do think it is a waste of tissue, which is a precious resource. I usually try to combine a DSAEK procedure with a lamellar graft for keratoconus so that I can use two pieces of a single cornea.
Dr. Gorovoy: That’s true. In some cases, I have even been able to use one donor cornea for three procedures. I use the posterior portion for DSAEK, the scleral rim for scleral grafts associated with shunts, and the anterior portion for an anterior graft. Even when I don’t need the anterior portion, I don’t discard it. I save it for about a week so that I have emergency tissue in reserve in case of a corneal perforation.
Q: From a business or efficiency perspective, does it make sense to use pre-cut tissue?
Dr. Gorovoy: The eye banks charge significantly more for pre-cut tissue. In fact, the cost can be 50% to 100% of the surgical fee for the entire procedure. I can understand that some surgeons feel they cannot justify an "unrecoverable" cost (the device) when the price of the more-expensive pre-cut tissue is passed through to Medicare or other third-party payers, as it typically is in the United States. However, I am not sure how long these pass-throughs will last if tissue costs increase. Some of the new managed care and Medicare HMOs have already introduced a global fee for the procedure that includes the tissue cost. In that scenario, it makes much more sense to buy your own system and do the dissections yourself.
Dr. Busin: In Europe, pre-cut tissue costs much more than a standard donor cornea, and it really is not cost-effective in the long run. Our reimbursement system pays a fixed amount per procedure, no matter how much you pay for the tissue. If tissue is too expensive, the costs of the procedure may be higher than the reimbursement and the hospital may choose not to let the surgeon perform this type of surgery. In addition, with the Moria DSAEK system, you can do a lot more than just DSAEK. Having the system gives you the flexibility to use it for deep anterior lamellar keratoplasty, for example. Honestly, I just would not feel like a complete corneal surgeon without the equipment necessary to perform DSAEK and anterior lamellar procedures.
Dr. Gorovoy: I agree. It is certainly advantageous to have your own machine and be able to use it for multiple procedures. I would add that for surgeons new to DSAEK, a hands-on O.R. course and mentoring from an experienced surgeon are critical. The procedure is not technically any more challenging than a penetrating keratoplasty, but there is a learning curve to perfect one’s technique and reduce rates of dislocation, endothelial damage and graft failure. Even in the midst of this learning curve, however, you and your patients can enjoy results that are dramatically superior to PK. OM
| Mark S. Gorovoy, M.D., (at left) is in private practice at Gorovoy Eye Specialists in Fort Myers, Fla. Contact him at (239) 939-1444 or mgorovoy@gorovoyeye.com. He has no financial interest in any product mentioned in this article. Massimo Busin, M.D., is in private practice in Italy. Contact him at +011-39-347-24-49-343 or mbusin@ yahoo.com. He has a non-financial consulting relationship with Moria. |


|