







Managing Failing Blebs
Surgeons describe how needling revision can improve trabeculectomy outcomes.
BY LARISSA CAMEJO, M.D., AND ROBERT J. NOECKER, M.D., M.B.A.
When a glaucoma patient demonstrates progression despite maximally tolerated medical and laser therapy, he must undergo glaucoma surgery. Frequently, trabeculectomy with or without adjunctive antimetabolites is the first line of treatment. Unfortunately, a significant percentage of trabeculectomies fail; this failure can occur early or late in the postoperative course. Certain risk factors have been identified as reasons for failure: African-American heritage, aphakia, youth, history of bleb failure, intraocular inflammation and intraocular surgery, among others.
This article will review considerations surgeons should take into account and techniques they should follow to manage a failing trabeculectomy successfully.
Know the Signs
The most important step in the management of a failing bleb is to recognize its presence. Bleb failure is preceded by a gradual increase in IOP and a change in the bleb's appearance. On slit lamp examination, the bleb can appear less diffuse, less elevated or flat or relatively avascular and opalescent. Alternatively, it can also appear very elevated and surrounded by a fibrotic vascular ring. The latter description characterizes the appearance of a Tenon's cyst or encapsulated bleb (Figure 1A and 1B). When evaluating bleb function, the physician must observe the bleb's overall appearance and look for microcysts, which indicate good filtration. These are easier to see with fluorescein stain. It is also important to measure IOP and to evaluate if pressure decreases after digital ocular pressure (DOP) is performed.
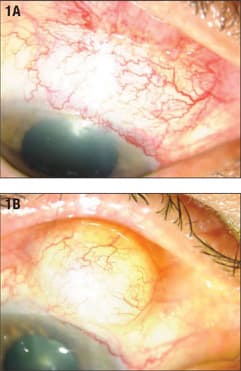
Figure 1. Examples of failing blebs. Figure 1A shows a limbal-based bleb that appears flat and is surrounded by thick vessels. Figure 1B represents an example of an encapsulated bleb or tenon's cyst. The bleb is markedly elevated and well delineated.
ALL IMAGES COURTESY OF THE AUTHORS.
The cause of bleb failure should be sought out. A careful gonioscopic examination must be performed to determine the patency of the sclerectomy site. The iris, ciliary body or vitreous can prolapse into the ostomy and occlude it. Nd:YAG laser can be applied to the iris-sclerectomy adhesion or vitreous to reopen the site. Nevertheless, the most common cause of bleb failure is episcleral fibrosis. Bleb leaks and blebitis are important conditions that should always be ruled out as well, as they require immediate care. It is important to evaluate the elevation of the bleb, the IOP and the depth of the anterior chamber every time you check a bleb's appearance. If a bleb leak is present, most likely, the bleb will be low, the chamber shallow and the IOP low.
Dealing With High IOP
Digital ocular pressure can be tried at the slit lamp when IOP is high. DOP may be applied as early as postoperative day 1. This is safer than cutting or releasing a suture at this point. DOP is performed by placing steady pressure over the inferior sclera, through the eyelids for 10 to 15 seconds. Pressure can also be placed superiorly behind the scleral flap and also through the eyelid, while asking the patient to look down. DOP will push aqueous through the sclerectomy into the subconjunctival space, thus lowering the pressure.
After the first, or better yet second, week postop, laser suturelysis (LSL) of the scleral flap sutures can be performed if IOP is still higher than target. For this, argon or green light laser and a Hoskins lens are used with the following settings: 400 mW, 0.01 seconds and 50 μm. LSL should be performed one suture at a time.
We routinely place two 10-0 nylon sutures on the scleral flap and therefore can perform two LSLs. Alternatively, if releasable sutures are placed intraoperatively, they can be released at this time. DOP can also be applied when a bleb is failing at a later time and, with careful instruction, can be taught to the patient so that he can perform the technique at home. DOP should be intermittent, allowing for several cycles, each lasting 10 to 15 seconds. This can allow for bleb remodeling by continuously forcing aqueous into the subconjunctival space.
When trying to restore bleb function, it is important to use frequent anti-inflammatories such as prednisolone acetate. Pressure-lowering topical therapy can be reinstituted as well. This may be less than ideal, considering that suboptimal adherence to medical therapy is frequently one of the contributing indications to advance therapy in the first place. Nevertheless, in certain cases it is worthwhile to treat with aqueous suppressants along with frequent prednisolone acetate as a temporary measure in an attempt to slow the healing process and allow for remodeling.
Sometimes, despite all our efforts, IOP may remain elevated. If this is the case, bleb needling can be performed as an alternative to surgically revising the bleb, repeating the trabeculectomy or implanting a tube shunt. Bleb needling will only work if the cause of bleb failure is episcleral fibrosis.
History of Bleb Revision
Bleb revision was first described by Ferrer1 in 1941. He described conjunctival dialysis as a procedure that consisted of incising the scar tissue and then separating the conjunctiva from the sclera with a spatula. Later, Pederson and Smith2 reported 69% success in needling encapsulated blebs, but noted that a high percentage of the eyes also underwent medical therapy. As ophthalmologists began administering antifibrotics during glaucoma surgery, reports of the agents' use in bleb needling appeared.
Ewing and Stamper3 were the first to describe the use of 5-fluorouracil (5-FU) in bleb needle revisions. They performed subconjunctival injections of 5-FU during the postoperative period and reported a 91.6% success rate with 63.6% (11 of 12 patients) requiring adjunctive medications. Shin et al4 administered single injections of 5-FU at the time of bleb needling and reported an 80% success rate (24 of 30 patients) with the IOP controlled in 21% of those eyes without additional medications. They also noted higher success with longer intervals between trabeculectomy and additional needling.
In 1996, Mardelli et al.5 described bleb needling as a slit-lamp procedure using injections of mitomycin C (MMC). They reported an overall success rate of 92% and commented that raised, quiet blebs responded better than inflamed, injected blebs. In their retrospective study, Shin et al.6 found three significant risk factors for failed 5-FU needling: An IOP greater than 30 mm Hg before needling; no MMC used during previous trabeculectomy; and an IOP greater than 10 mm Hg immediately after needling.
Broadway et al.7 studied the use of 5-FU prospectively and reported that an immediate reduction in IOP to less than 11 mm Hg was favorable to the long-term efficacy of bleb needling. Recently, Gutierrez-Ortiz et al.8 published a prospective study showing that MMC needling was more successful if performed within 4 months of trabeculectomy. Comparing studies is challenging due to variations in inclusion criteria and definitions of success as well as the low number of prospective, randomized and controlled trials on the subject.
Our Technique
Surgeons may perform a needling revision in the OR or in their offices. The OR offers the advantage of a more controlled setting and may allow for more extensive treatment. Nevertheless, we routinely needle blebs in the office at the slit lamp and believe the procedure may be executed with a high level of success and minimal to no patient discomfort. The main advantage of an office procedure is to avoid another visit to the OR.
While there are many ways to needle a bleb, we will describe our preferred technique below.
After obtaining informed consent, we administer a drop of a fourth-generation fluoroquinolone followed by a generous application of topical lidocaine 2% gel over the bleb to be needled (intraoperatively, we reapply the gel as needed). We then wait 5 minutes, during which time a nurse draws 0.1 mL of MMC 0.04 mg/mL into a 1-mL tuberculin syringe. We should note that this concentration is 10 times lower than what we typically use during the primary procedure. Surgeons should ensure that they have received the correct concentration of MMC from their pharmacy.
With the patient seated at the slit lamp, we place a sterile lid speculum and inject the MMC subconjunctivally with a 30-gauge needle, which enters the conjunctiva, posteriorly directed, bevel up approximately 5 to 10 mm from the bleb site. Normally, we perform the injection from the temporal side of the bleb for an easier approach. We distribute the MMC with the aid of a cotton swab by applying pressure in a rolling motion over the conjunctiva next to the injection site.
After removing the lid speculum, we place a 25-gauge needle on a 1-mL syringe and use its cap to bend the needle at its base to approximately 60°. Fifteen to 20 minutes after injecting the MMC, we replace the lid speculum and re-enter the subconjunctival space at the same location. We introduce the needle bevel up and move it back and forth in an attempt to disrupt all scar tissue in the sub-Tenon's space. Our aim is to improve the flow posteriorly, so we puncture the wall of the bleb multiple times, especially posteriorly, away from the limbus. The goal of the procedure is to increase the permeability of the bleb's wall and therefore produce a more diffuse, better functioning bleb. We keep the needle bevel up over the scleral flap and are extremely careful not to create a conjunctival buttonhole.
Multiple passes of the needle are typically necessary to revive the bleb. Ideally, all of the needling is performed from a single site, but it is sometimes necessary to approach the bleb from both sides (temporally and nasally). If the maneuver is successful, the bleb will change its appearance during the procedure. Specifically, flat blebs will grow more elevated, and encapsulated blebs will become more diffuse. The bleb's changing appearance indicates the restoration of aqueous flow. (Figures 2-5).
In some cases, it is necessary to lift the scleral flap with the needle and enter the anterior chamber to restore the flow of aqueous. This situation may arise if the bleb is flat with a visible scleral flap and does not respond to episcleral needling. The surgeon will lift a scarred-down scleral flap, if it is the main cause of resistance. At the end of the procedure, we instill fluorescein to check for bleb leaks. Holding a cotton swab in place for 1 minute usually stems leakage at the injection site.
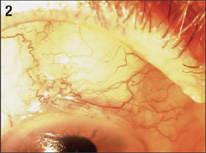
Figure 2. Preoperative appearance of a failing bleb.
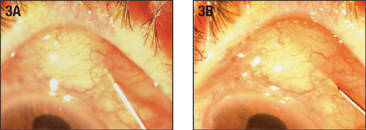
Figure 3A. Needling procedure. A 25-gauge needle is introduced bevel up into the bleb and is directed towards the posterior border in an attempt to dissect the episcleral fibrosis. Figure 3B. The needle is moved back and forth repeatedly.
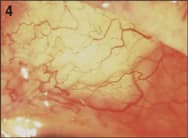
Figure 4. Appearance of the bleb shown in Figure 2 after successful needling.
We also measure the IOP. Low pressures are promising. Several studies have found a correlation between an immediate reduction in IOP to less than 11 mm Hg and a higher rate of success.6-8 Postoperatively, we prescribe prednisolone 1% q.i.d. and follow up with the patient in 1 week. We normally see the patient every 1 to 2 weeks until a stable, well-functioning bleb is present.
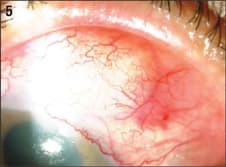
Figure 5. Appearance of the bleb shown in Figure 1B after successful needling.
We repeat needling with MMC up to three times, depending on the initial response. In most if not all studies, success was achieved with more than one needling procedure. It may also be a good idea to draw unpreserved lidocaine 1% after MMC so that the lidocaine is injected first. This is for both for anesthetic purposes and to create a wheal (or elevated region of conjunctiva) under which to safely inject the MMC. Surgeons may use other needles from 25- to 30-gauge for this procedure. We favor the 25-gauge needle because it is sturdier and more resistant to bending during the disruption of scar tissue.
In addition, surgeons have proposed using medications other than MMC and 5-FU. Tham et al.9 conducted a pilot study on intrableb injections of triamcinolone-acetonide after bleb-forming glaucoma surgery and Kahook et al.10 published a case report on the subconjunctival injection of bevacizumab (Avastin, Genentech) in encapsulated blebs. Additionally, Iwach et al.11 suggested the transconjunctival administration rather than subconjunctival injection of MMC.
We prefer MMC over 5-FU primarily because we feel that it is more comfortable to the patient and less toxic to the corneal epithelium. We also feel that MMC is more potent and effective than 5-FU and requires fewer follow-up injections.
A Procedure Worth Learning
Although less invasive than trabeculectomy, bleb needling should be performed with caution. Possible complications include hyphema, a flat anterior chamber, choroidal effusions, conjunctival buttonholes and endophthalmitis.2,5,8 Nonetheless, needling can be an effective means of rescuing failing procedures and can delay or prevent a return to the OR. Despite many variations in the technique and adjunctive medications used for bleb needling, surgeons can improve their outcomes with trabeculectomy if they follow guiding principles such as those outlined in this article. OM
References
- Ferrer H. Conjunctival dialysis in the treatment of glaucoma recurrent after sclerectomy. Am J Ophthalmol. 1941;24:788-790.
- Pederson JE, Smith SG. Surgical management of encapsulated filtering blebs. Ophthalmology. 1985;92:955-958.
- Ewing RH, Stamper RL. Needle revision with and without 5-FU for the treatment of failed filtering blebs. Am J Ophthalmol. 1990;110:254-259.
- Shin DH, Juzych MS, Khatana AK, et al. Needling revision of failed filtering blebs with adjunctive 5-fluorouracil. Ophthalmic Surg. 1993;24:242-248.
- Mardelli PG, Lederer CM Jr, Murray PL, et al. Slit-lamp needle revision of failed filtering blebs using mitomycin C. Ophthalmology. 1996;103:1946-1955.
- Shin DH, Kim YY, Ginde SY, et al. Risk factors for failure of 5-fluorouracil needling revision for failed conjunctival filtration blebs. Am J Ophthalmol. 2001;132:875-880.
- Broadway DC, Bloom PA, Bunce C, et al. Needle revision of failing and failed trabeculectomy blebs with adjunctive 5-fluorouracil: survival analysis. Ophthalmology. 2004;111:665-673.
- Gutierrez-Ortiz C, Cabarga C, Teus MA. Prospective evaluation of preoperative factors associated with successful mitomycin C needling of failed filtration blebs. J Glaucoma. 2006;15:98-102.
- Tham CC, Li FC, Leung DY, et al. Intrableb triamcinolone acetonide injection after bleb-forming filtration surgery: a pilot study. Eye. 2006 [Epub ahead of print].
- Kahook MY, Schuman JS, Noecker RJ. Needle bleb revision of encapsulated filtering bleb with bevacizumab. Ophthalmic Surg Lasers Imaging. 2006;37:148-150.
- Iwach AG, Delgado MF, Novack GD, et al. Transconjunctival mitomycin-C in needle revisions of failing filtering blebs. Ophthalmology. 2003;110:734-742.
| Larissa Camejo, M.D., is assistant professor at the Department of Ophthalmology at the University of Pittsburgh and the director of the University of Pittsburgh Medical Center Eye Center-Bethel Park. Dr. Camejo reports no financial interests. She may be reached at (412) 647-2152 or via e-mail at camejol@upmc.edu. |

|
| Robert J. Noecker, M.D., M.B.A., is the director of the glaucoma service and associate professor/vice chair at the Department of Ophthalmology at the University of Pittsburgh. Dr. Noecker is a consultant for Allergan, Alcon, Merck, Lumenis, Heidelberg and Ista Pharmaceuticals. Dr. Noecker may be reached at (412) 647-2152 or via e-mail at noeckerrj@upmc.edu. |

|