







Vital Signs: How to Monitor and Improve the
Performance of Your Practice
These six steps can help build a
more successful
practice.
BY KAY
COULSON
How many times in your practice have you asked, "How are we doing? Are we growing? Are we profitable? Can we perform better? Are we focused on the correct issues?" Ophthalmologists are extremely effective in diagnosing a patient's problem and prescribing a cure. But how effective are you and your administrators in assessing the health of your practice? Are you accurate in diagnosing problem areas? Do you prescribe solutions to ensure a vibrant and growing business? How effective are you in delivering business "outcomes," or practice success? How much time do you spend on "enhancement" or reacting to practice problems?
These were the questions I pondered when opening a refractive center in mid-2001. In the post-September 11th environment of declining LASIK interest and reluctant discretionary spending, any benchmarks I had gleaned from the early go-go years of LASIK no longer applied. So instead of looking outward to find "the answer," I looked inward and asked some very fundamental questions:
-
What type of practice do we want to build?
-
How do we structure our staff, service lines and protocols to deliver this vision?
-
How will we measure success?
-
How will we forecast effectively so that we always act from a position of strength, rather than react from a position of weakness?
What follows are six "Vital Signs" discerned and refined through the building of this first practice — InSight LASIK in Colorado — a purely refractive center we opened shortly before 9/11 in a very competitive LASIK market. I have since applied this same method to a 25-year old, well-respected, strongly surgeon-branded, multi-specialty practice in Louisiana and achieved similar results.
What Do You Want To Be?
To begin, answer a simple question, "What type of practice am I trying to build?" A general ophthalmology practice? Comprehensive surgical practice? Cataract-only practice? LASIK and lens practice?
Assume you want to build a surgical practice focused on treating LASIK and lens patients. The fuel — the appointment type that will build this practice — is LASIK and lens consultations. Annual eye exams, glaucoma checks and an optical department are not fuel. They are distractions that quickly fill an appointment calendar, but they will not help achieve your goal. How did they come to dominate the schedule? Probably when you started to practice, you scheduled everyone who called. As new techs or optometrists were added, annual exams, contact lenses and optical were incorporated to fill their time. Exams then uncovered glaucoma or retina issues and you decided not to refer these out. Past LASIK or cataract patients requested annual exams. Before you knew it, 10 years had past and you had built a general ophthalmology practice, not the specialty surgical practice you had envisioned. You are now seeing 80 patients per day, employing a small army to code and bill, performing surgery only 1 day per week, and feel like most of the LASIK and all of the elective lens patients are going elsewhere.
Yet a specialty practice is just that — special. It has a narrow focus. For the sake of this article we will assume you want to build a strong LASIK and elective lens surgical practice. Now, let's see where you are, where you would like to be and how we will bridge the gap.
Where Are You Today?
How many people called or inquired about LASIK or lens surgery from you in the last 4 weeks? How many consultations for LASIK or lenses were performed? And how many LASIK or lens surgeries did you perform? In my experience, practices performing elective procedures are doing well if one out of two people inquiring go on to surgery on a rolling 52-week basis. If your practice is in balance, 100 new inquiries per month should generate 100 procedures per month and 200 inquiries should yield 200 procedures. Yet what I often see in offices struggling with efficiency and profitability is a practice generating 200 inquiries per month, but only doing 100 procedures. The key is determining where within your "refractive funnel" (Figure 1) the problems reside.
|
|
|
|
Figure
1. The "Refractive Funnel" identifies optimal conversion levels and allows you to
diagnose where in your system problems lie.
|
|
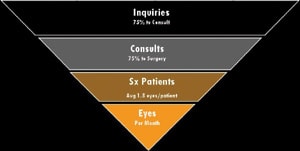
Vital Sign #1: Inquiries
Interest in your practice is defined by inquiries. Every practice looks for a balance between the quantity of inquiries received, and the quality of those inquiries. Inquiries include phone calls, walk-ins and current patients interested in a new service. Inquiries do not include names that are gathered by "giveaways" or offering anything for free.
Good quality inquiries can be converted to consult 75% of the time, if staff training and phone protocol are well-developed, fees are reasonable and the practice reputation is strong within the market. Once this 75% conversion benchmark is established, gradually expand marketing reach to increase your call volume. The wider your net is cast, the harder it will be to convert, so it is important to adjust marketing activities slowly to continually maintain conversions at 75% or greater.
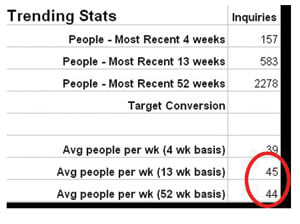
I also advise setting a target for weekly inquiries and communicating this to your staff. This target is determined by working backwards from the number of procedures you desire in a given month (Figure 2). For example, the following formula can be used:
100 eyes/1.8 eyes per person/75% consults to surgery/ 75% inquiries to consult = 100 Inquiries Needed
Track the practice segments you intend to grow — LASIK, elective lenses or cataracts. Monitor the inquiries for these service lines weekly. Track practice totals on a monthly, quarterly and annual basis so you can assess progress. Finally, share this information with your staff each week, via email or at a staff meeting.
|
|
|
|
Figure 2. This practice, averaging 45 inquiries
per week, should be performing 200 surgeries per month if operating effectively
under the 75%/75% conversion model.
|
|
Vital Sign #2: Conversion
Conversion is a two-part process defined by the number of inquiries who actually convert to surgery (Figure 3). Part 1 of the conversion process includes the number of inquires who attend a consultation. An efficient practice generating quality inquiries should convert 75% of inquiries to consults. Part 2 of the conversion is the number of consults who attend surgery. An effective practice should convert 75% of consults to surgery.
Conversion should not include no-shows or cancellations at any level. If a practice has more than 5% no-shows on any given day, the reminder system should be improved. Options include making reminder calls if the practice is not already doing so, making calls before 10 a.m. the day before the consultation and performing reschedule calls within 2 hours of the missed appointment.
Assess the inquiries-to-consult ratio on a 4-week basis, since most practices do not book further out than this. If your practice does book further out, consider adding another counselor. Patients with inquiries will not wait more than a week, rather, they will call another practice. We perform consults 4 days per week, so our front desk knows if they do not see six to eight yellow appointments booked each day, they need to leave room in the schedule to accommodate new inquiries. They are aware that patients coming in for postoperative visits and measurements cannot overrun the schedule.
If your inquiry-to-consult ratio is lower than 75%, first improve phone intake and protocol with staff, then evaluate marketing placement and creative. If these elements are strong, evaluate fees. Even great marketing and well-trained staff cannot overcome pricing that is viewed by patients as too high relative to outcome delivered within the market. Conversely, if you desire fees 25-50% higher that the average rate in your market, accept a conversion target lower that 75%.
If your consult-to-surgery ratio is lower than 75%, train counselors/doctors, reassess competition and improve proof of excellence. Track reasons for not scheduling and train staff on how to adapt or respond.
Conversely, if your consult-to-surgery ratio is higher than 90%, consider price increase. Converting too well indicates your value equation is too strong.
|
|
|
|
Figure 3. Phone staff is evaluated on their
inquiry-to-consult ratio over 4 weeks, since this practice attempts to schedule
inquiries within one week of contact. Patient counselors are evaluated on their
consult-to-surgery ratio over 13 weeks to allow for surgery bookings that can range
for 2 weeks to 2 months out, depending on patient stability.
|
|

Vital Sign #3: Pipeline
Pipeline represents who will be visiting the practice in 60 days. The phone must ring and you have to develop programs to ensure this happens. Pipeline is the tool that signals when to dial-up or dial-back marketing activity. It is the tool I use to know today what procedure volume we will have next month. Using this tool effectively will mean no surprises, more efficient staffing and better management of cash flow.
How full should the pipeline be? This varies based on the seasonality of refractive surgery in your market. My rule-of-thumb is to maintain a pipeline of at least a half month of eyes. If you desire 100 eyes per month, your pipeline should hold 50 eyes or you need to dial-up the marketing.
Ultimately, the pipeline should equal future consults booked multiplied by the number of eyes per patient multiplied by consult conversions (Figure 4).
|
|
|
|
Figure 4. This practice has 60 consults on
the books that have not yet been seen. At their conversion ratio of 78% and averaging
1.8 eyes per patient, there are 84 eyes in the pipeline that are not yet on the
books as surgery but will be based on historical trends.
|
|

Vital Sign #4: Referrals
Referrals are proof of great service. You must deliver a great outcome. In today's LASIK and lens exchange environment, a great outcome is the cost of entry, not a determining factor in whether a person chooses your practice. Now that LASIK has achieved mainstream acceptance, a referral is much more difficult to secure. People know they want LASIK, but they perceive surgeons and centers as interchangeable.
To maximize patient referrals, a practice must excel at all phases of customer service: how the phone is answered, how the office looks, how customers are treated at the consult, how staff bonds with patients over several preoperative and postop visits and finally, how good patients' result are. Today's patient does not want just a good outcome. They expect a great experience.
Assess referral volume by capturing the specific name of the past patient that referred this current patient. Abolish word-of-mouth as a referral source in your marketing tracking. When asking, "What prompted you to call us today?" get a specific name. Ask, "Was it a patient who told you about us? Someone who saw us for a consult? A friend of a past patient?" People will not mind if they are asked.
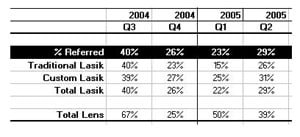
Referrals equal the percentage of surgery patients that come from past surgery patients. A practice's target should be 25% or more (Figure 5).
What if referrals fall below 25%? Check your thank-you cards or gifts — are they motivating? Check the timing — are you delayed in sending thanks for referrals? Check outcomes. If your results are not outstanding, patients will not refer.
|
|
|
|
Figure
5. Referrals = % of surgery patients that come from past surgery patients. Target
= 25%+.
|
|
Vital Sign #5: Practice Efficiency
How do you know if your practice is efficient? If you have the correct appointment mix? The right staff level? How do you know if patients are being seen enough or too much? How do you plan for seasonality? How do you control appointment mix so that the calendar has room for consults and surgeries? How do you know, when the staff says they are working too long or seeing too many patients, if it is true? A practice efficiency report answers these questions and assists you in managing day-to-day patient flow and staff issues (Figure 6).
The following benchmarks hold true for both of the practices I've guided:
-
Five or more consults per day (25 per week), allow us to achieve our minimum volume goals.
-
Consults should make up 20% to 25% of total appointments.
-
If postops visits make up more than 45% of total appointments, we have an outcomes/enhancement issue.
-
One MD or OD and one COT can handle 20 to 25 appointments per day.
|
|
|
|
Figure
6. Practice efficiency report.
|
|
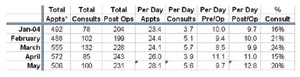
Determine the number of consults you need to achieve your volume goals. Make sure postop visits are not over-running your schedule. If you plan to see patients five times postoperatively but appointment analysis indicates you are seeing them nine times, you need to sit down with your doctors. Determine if you are seeing people because you have a problem, or because the doctor has a hard time releasing patients.
Be on the lookout for any increase in postop visits. This might mean laser servicing is in order, your nomogram needs to be revisited, there is an infection issue, biometry is poor or outcomes need to be updated.
Vital Sign #6: Marketing Efficiency
|
|
|
|
Figure
7. This practice in 2002 had poor consult to surgery conversions, driving the cost-per-surgery
to $550 per eye. By adjusting fees and realigning marketing spending, the cost-per-lead
and cost-per-surgery were substantially improved, greatly improving practice profitability.
|
|
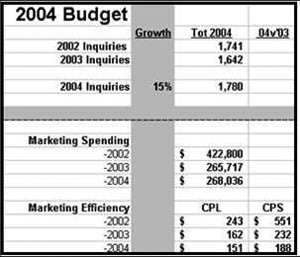
Marketing efficiency is measured through two components — cost-per-inquiry and cost-per-surgery (Figure 7). If your practice is established and well-functioning, and assuming the 75%/75% conversion model, the following benchmarks drive marketing spending.
Determine how many leads have been generated, and at what cost for the prior year. Project how many leads must be generated this year to achieve volume goals. Calculate cost-per-lead for the prior year and coming year. If marketing dollars are working effectively, cost-per-lead should be below $200.
Calculate cost-per-surgery. If conversions are strong and the practice is optimizing conversion of all leads, cost-per-surgery should be just slightly higher than cost-per-lead. Determine the marketing budget for the upcoming year by calculating the cost-per-lead multiplied by the amount of required leads. This will provide an optimal marketing budget. For example, if your target is 100 procedures per month, and conversions are efficient at 75% inquiry to consult and 75% consult to surgery, you need to generate 100 inquiries. At a cost-per-inquiry of $180, you should budget $18,000 per month for marketing.
Assess the efficiency of your marketing by breaking leads down by referral source. Utilize various media to combine brand awareness vehicles with inquiry-generating vehicles, but do so with the cost per lead in mind. Be sure to think about marketing in terms of referral channels, such as direct patients, comanaged patients and facility patients generated by visiting doctors, and develop specific marketing programs for each.
What have I learned using the Vital Signs assessment method with two very different ophthalmology practices over the last four years? Capture performance data accurately, diagnose trouble correctly, prescribe treatment to achieve success and monitor compliance to ensure growth. These steps build the profitable, satisfying practice you envision.
Kay Coulson, founder of Elective Medical Marketing and director of the Alcon-sponsored course Refractive Excellence, assists Ophthalmologist in the development of their elective vision practices. She can be reached at kay@electivemed.com.