







Your Options in VISCOELASTICS
With so many new procedures emerging, including bimanual phaco, endocyclophotocoagulation, nonpenetrating glaucoma surgery, phakic IOLs, and refractive lens exchange, it's likely that new viscoelastic agents to complement them will be developed. In the meantime, for your convenience, we've listed today's state-of-the-art products here, with a focus on their uses in cataract surgery.
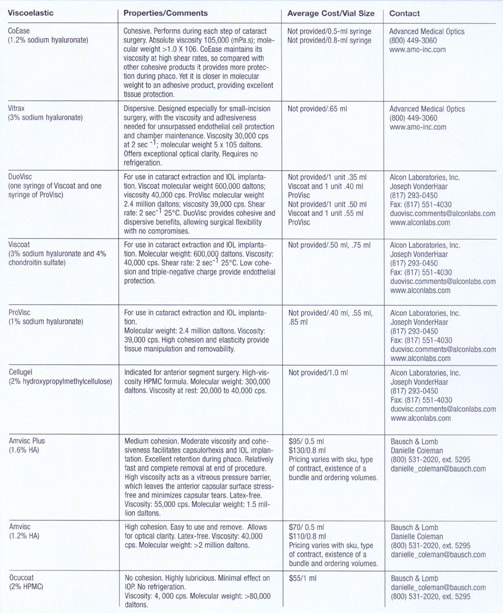
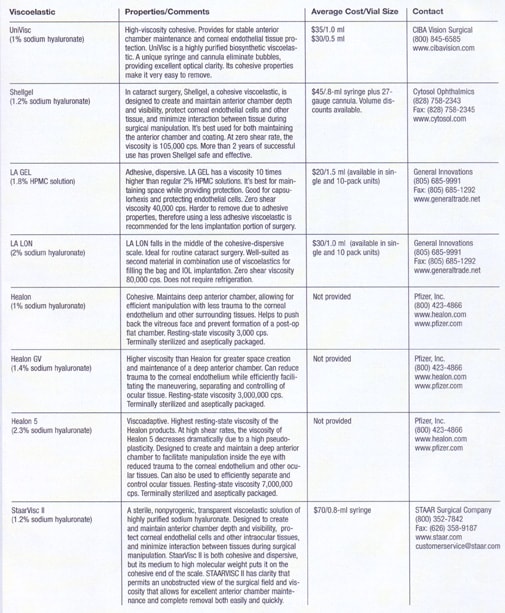
The information in this chart was provided to
Ophthalmology Management by the viscoelastic manufacturers. It was not
reviewed or verified by Dr. Arshinoff.
Recent Trends in OVDs
BY STEVE ARSHINOFF, M.D., F.R.C.S.C.
In this article, I would like to draw attention to a few of the recent and upcoming innovations in Ophthalmic Viscosurgical Devices (OVDs).
Historically, cataract surgical strategies were based simply upon filling the anterior chamber (AC) with an OVD, and then proceeding with a relatively straightforward procedure. But cataract surgery did not stand still, and new techniques, different preferred phaco settings, and new IOL designs were better served by new approaches.
|
|
|
|
When we consider cohesion, we see that we still have many areas of possible OVD development to
explore. |

The Ultimate SST
The dispersive-cohesive viscoelastic soft shell technique (SST) that I developed appeared to have sufficient variations to approach any circumstance. Then, viscoadaptives came along, allowing us to think that perhaps a single molecule might be sufficient to create and protect surgical spaces, pressurize the anterior chamber sufficiently, permit partitioning of the AC into a protected space and an active surgical space, where BSS could circulate freely, to deal with complications.
Viscoadaptives function beautifully, but sometimes it is difficult to perform a capsulorhexis in a very viscous environment, or to perform hydrodissection when the AC is full of viscoadaptive. Furthermore, removal of viscoadaptives can be more difficult in the presence of modern sharp-edged IOls, on which viscoadaptives fracture, leaving some OVD behind the IOL, and making removal more difficult.
To resolve these concerns, I developed the ultimate soft shell technique (USST), which uses BSS with a viscoadaptive. The substitution of non-preserved isotonic lidocaine for BSS in the USST allows us to do phacoemulsification without cycloplegics, permitting nearly full functional visual recovery within 15 minutes of surgery. USST filling of IOL injectors prevents evaporation of the OVD between the time of filling the cartridge and insertion of the IOL, resulting in less resistance, fewer cases in which the IOL is unintentionally damaged in insertion, and smoother IOL implantation.
Complex surgical cases can be performed more safely by combining techniques. For example, if the SST and USST are combined in cases of Fuchs' Endothelial Dystrophy, the case can be performed with absolutely zero BSS flow against the endothelium. I achieve this by first forming a mound of Viscoat on the lens surface, followed by filling the AC 75% with Healon5, injecting it beneath the Viscoat to push the Viscoat up against the endothelium. I then inject BSS below the Healon5 to form an aqueous layer overlying the lens capsule. Phacoemulsification is performed with the flow rate reduced to 20 cc/min, with all work done in the capsular bag. The Healon5 and Viscoat remain undisturbed. At the end of the case, I remove the Healon5, but leave the Viscoat undisturbed. I place Pilopine 4% gel in the conjunctival cul de sac to prevent postoperative IOP spikes.
This type of modification of the USST is also helpful with bimanual phaco, where the position of the irrigation cannula often results in excessive irrigation of the endothelium.
The USST also enhances implantation of phakic IOLs. The IOL is placed behind the OVD, so that it can open in a deep, stable chamber, and OVD removal from behind the IOL is not an issue. Alternatively, we can use OVDs that are less-viscous than viscoadaptives for easier removal following phakic IOL implantation.
Plenty of Possibilities to Explore
There are many ideas on the horizon in OVD development. At the ASCRS meeting in 2002, Thierry Amzallag, M.D., presented the idea of adding low concentration sodium hyaluronate to the irrigating solution. Other OVD polymers may also be tried, and this remains an unexplored area with obvious potential benefit.
When we take cohesion into consideration, (See chart above.), we see that there remain many unexplored areas of possible OVD development. Undoubtedly, future research will explore these areas, and we will examine the surgical utility of these new potential OVDs as they are developed.
Rheology, the science of fluid flow, is the scientific foundation of phacoemulsification surgery, and of OVD development and use. Fluids may range in properties from air to glass, and may flow like the wind, or change minimally over centuries as seen in the windows of ancient Italian churches. OVD potential is limited only by our imagination and our exploratory efforts.
Dr. Arshinoff is a clinical instructor at the University of Toronto and in private practice at York Finch Eye Associates, also in Toronto.