







rx
perspective
The Evolution of Alpha2-Agonists
This versatile class of glaucoma drugs has come
a long way and has a lot to offer.
By Thomas W. Samuelson, M.D.
Although many ophthalmologists have embraced prosta-glandin and prosta-mide products as first-line choices for glaucoma therapy, alpha2-agonists deserve consideration as adjunctive agents, or as first-line treatment for patients who can't tolerate prostaglandin or prostamide agents (hypotensive lipids). Beta-blockers, prostaglandins and prostamides are more potent, but alpha2-agonists effectively reduce IOP, with fewer and milder side effects. Alpha2-agonists are versatile, and they've been proven effective in nearly all glaucomas.
The newer formulations of alpha2-agonists have a primary affinity for alpha2 receptors; they activate the receptors presynaptically, inhibiting the release of norepinephrine. When administered two or three times a day they effectively reduce the formation of aqueous humor, and the decrease in aqueous flow causes a reduction in IOP. After prolonged treatment, they also produce an increase in uveoscleral outflow (Toris, Am J Ophthalmol 1999).
Here I'd like to provide a brief summary of how this class of drugs has evolved over the years, along with some advice for using these drugs for maximum effectiveness.
The First Generation
The first of the alpha2-agonists used to treat glaucoma was clonidine, a systemic, centrally acting anti-hypertensive medication. Al-though it was approved in some European countries as an ophthalmic topical medication to lower IOP, it had a serious drawback: Clonidine readily crosses the blood-brain barrier and lowers blood pressure. This limited its use in glau- coma patients and prevented it from gaining approval in the United States, despite its ocular efficacy.
However, the fact that it worked so well in the eye spurred further investigation of this drug class. The result was the development of apraclonidine 1%, a polar derivative of clonidine that was found to cause fewer systemic effects. Apracloni-dine was eventually approved to control or prevent post-surgical elevations in IOP.
Today, apraclonidine is frequently used perioperatively to blunt any pressure rise following argon laser trabeculoplasty, Nd:YAG laser iridotomy, or Nd:YAG laser posterior capsulotomy. Also, apraclonidine 0.5% has been approved for use as an adjunctive therapy for patients who are already using maximally tolerated glaucoma therapies.
Apraclonidine is indicated for short-term use, primarily because tachyphylaxis has been seen within the first few months of use. Ocular allergies also limit apraclonidine's usefulness: As many as 15% to 48% of patients experience an allergic reaction (Cantor, Exp Opin Invest Drugs 1997).
A Step in the Right Direction
Ironically, a second-generation alpha2-agonist, brimonidine 0.2%, was originally tested as a treatment for systemic hypertension. However, it was ineffective as a means to re-duce blood pressure, which made it a viable candidate to test in the eye.
The ophthalmic formulation was developed in the mid-80s as a highly selective alpha2-adrenergic receptor agonist (Burke, Surv Ophthalmol 1996). It had numerous advantages over the previous generation:
► Its relative affinity for alpha2 receptors is 23 to 32 times greater than that of apraclonidine (Fiscella, P&T Digest 2002).
► Brimonidine has a much lower affinity for alpha1 receptors; in fact, it's 1,700 times more selective for alpha2 receptors than alpha1 receptors. This improves efficacy.
► The increased selectivity for alpha2 receptors rather than alpha1 receptors reduces side-effects such as mydriasis, conjunctival blanching, eyelid retraction, and vasoconstriction (Burke, Surv Ophthalmol 1996). The concentration is sufficient to activate the alpha2 receptors in the ciliary body, but not the alpha1 receptors in the eyelid, iris, or posterior segment (Acheampong, Drug Metab Dispos 1995).
► No tachyphylaxis has been observed with brimonidine 0.2%.
Despite the fact that brimonidine 0.2% was considered to be an improvement over apraclonidine, it still had some characteristics that were less than ideal. Its use was linked to ocular allergies in some patients, and fatigue and dry mouth were still occasional limiting factors.
Developing a Better Formula
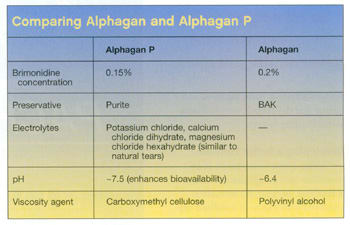
Today, a new formulation of brimonidine tartrate ophthalmic solution is available. Because the formula is preserved with Purite (a stabilized oxychloro complex) instead of the more widely used preservative benzalkonium chloride (BAK), it enhances safety and tolerability while still maintaining effective reduction of IOP.
Purite, which has a wide spectrum of antimicrobial activity, allows the formulation to remain stable at a higher pH (7.5). The higher pH results in improved bioavailability, so the concentration of brimonidine can be decreased to 0.15% without any loss of efficacy.
This has several important benefits:
► The new formulation is associated with significantly fewer ocular allergies (Katz, J Glaucoma 2002).
► BAK may be contraindicated entirely in the presence of trophic ulcers or other states of severely compromised corneal epithelial integrity (Noecker, Adv Ther 2001; De Saint Jean, Curr Eye Res 2000). The new formulation widens the range of circumstances in which brimonidine can be used.
► The patient's BAK exposure is reduced. Given that many patients use multiple glaucoma medications containing BAK several times a day -- sometimes for years -- the repeated exposure to BAK may well have a cumulative effect. Recent research suggests that BAK, even at very low concentrations, is toxic to lens epithelial cells and may be associated with cataract formation in patients over time (Goto, Arch Ophthalmol 2003; Noecker, Adv Ther 2001). Studies have also found that the preservative disrupts the blood-aqueous barrier in early postoperative pseudophakia and increases the incidence of angiographic cystoid macular edema in patients undergoing cataract surgery (Miyake, Arch Ophthalmol 2001).
While we await further research in these areas, from a practical standpoint it seems clear that the elimination of BAK from brimonidine 0.15% makes this the agent of choice within the alpha2-agonist drug class. (Characteristics of brimonidine 0.15% compared with brimonidine 0.2% are shown in the table to the right.)
All families of medicine that are used to treat glaucoma have limits in their application, but the alpha2-agonists are well tolerated and very versatile:
► An ophthalmologist may avoid using prostaglandins or prostamides when a patient has recently had surgery, or avoid the lipid family when a patient has inflammatory glaucoma. In contrast, the alpha2-agonists are eminently usable for all but infantile glaucomas.
► Because their action is local and not systemic, the alpha2-agonists are a safe alternative to beta-blockers.
► Their pronounced effect within 2 hours of dosing make alpha2-agonists particularly useful when the goal is to achieve a rapid and significant decrease in IOP. This is often the case in perioperative situations (for example, following laser trabeculoplasty or YAG capsulotomy).
Their rapid action and versatility notwithstanding, the alpha2-agonists tend to be less potent than other drug classes. For this reason, I believe the most likely use of brimonidine 0.15% is as an excellent adjunctive therapy. However it's also well-suited for use as monotherapy, in particular when:
► patients have mild glaucoma
► other agents have failed, either because of tachyphylaxis or because the patient simply didn't respond
► the patient is prone to inflammation
► the patient is concerned about the side-effects of lipids, such as eyelash growth, iris color change, or hyperemia.
One final note: When dosing with brimonidine Purite b.i.d., it's important to measure IOP at trough effect as well as at peak, to be certain that adequate reduction in pressure occurs throughout the day. If trough control isn't adequate, consider t.i.d. dosing, or adding a second agent.
The Evolutionary Advantage
As clinicians, we need all the agents and tools we can get to create the most appropriate treatment regimen for each patient. Fortunately, each new generation of therapy offers improvements over its predecessors, and further contributes to our therapeutic armamentarium. The evolution of brimonidine is certainly a case in point.
With this newest formulation, we've seen a substantial drop in the percentage of patients having an allergic response. We're also seeing fewer systemic side effects -- less fatigue and dry mouth -- as a result of enhanced bioavailability and lower concentration. All of these improvements over previous-generation alpha2-agonists are substantial, and they bode well for both our patients and our practices.
Dr. Samuelson has a consultative practice in Minneapolis and is clinical associate professor of ophthalmology at the University of Minnesota. He also directs glaucoma service at Regions Hospital and is a consultant for the Veterans Affairs Medical Center (VAMC). Dr. Samuelson has received the American Academy of Ophthalmology's "Achievement Award" honoring physicians who significantly contribute to the Academy's educational endeavors.