







Ophthalmic surgery continues to migrate from the hospital outpatient department (HOPD) to the ambulatory surgical center (ASC). For those of us building high-performance centers, minimally invasive glaucoma surgery (MIGS) is no longer an “add-on” service line, it is a core capability that directly impacts clinical outcomes, patient experience, and ASC economics. In 2026, updated Medicare reimbursement, evolving trial endpoints, and next-generation device approvals are changing how I think about building a cataract and glaucoma program that is both clinically excellent and operationally scalable.
When MIGS is implemented well, it is a true win for patients, surgeons, and the ASC. We address a growing glaucoma burden in an aging population; we preserve (and often improve) operating room (OR) throughput; and we create a meaningful contribution margin. The key is execution, understanding the clinical landscape, controlling device cost, engineering the intraoperative workflow, and scheduling/staffing with intention.
Integrating MIGS Into the ASC Model
The value proposition of MIGS in the ASC is straightforward. MIGS complements high-volume cataract surgery with minimal disruption, and it also stands on its own for patients who need pressure lowering without a cataract indication.
Synergy With Existing High-Volume Service Lines
Most MIGS cases are performed at the time of cataract surgery. Because phacoemulsification is the highest-volume procedure in nearly every ophthalmic ASC, the incremental operational burden of adding a MIGS step is usually modest provided the team is trained and the room is set up for intraoperative gonioscopy. In most centers, the required “capital” is already in the room: microscope, gonioprism, and standard instrumentation.
Shifting Care to the ASC
Historically, trabeculectomies and tube shunts lived in the HOPD because of longer case times and more variable postoperative courses. MIGS has shifted that equation. With predictable, microincisional techniques and a favorable safety profile, MIGS fits the ASC model: efficient turnover, reproducible timing, and lower resource variability without compromising patient safety.
Scheduling and OR Flow Optimization
Operational efficiency is the cornerstone of ASC profitability, and it’s often the first concern I hear from administrators: “Will MIGS slow down a high-volume cataract day?” In my opinion, the answer is a profound “No.” If you standardize the setup, anticipate the angle work, and keep device logistics tight, minimal adjustments to the schedule are required, and there are significant upsides to the incorporation of MIGS to our workflow.
Assessing the Workflow Impact
In my experience, most MIGS add-ons take 3-5 minutes and rarely require more than 8 additional minutes once the team is comfortable. When the room is prepared correctly, the impact on turnover is minimal. The delays I see are almost always “process” problems, not surgical ones.
- Intraoperative gonioscopy: This is where time is won or lost. Have the gonioprism on the field, confirm bed height early, and make head/microscope tilt a rehearsed step rather than an improvisation.
- Sterilization and instrumentation: If you rely on microinstrument trays, coordinate with the sterile processing department so tray turnover never becomes the rate-limiting step. Single-use platforms simplify this, but inventory control becomes more important.
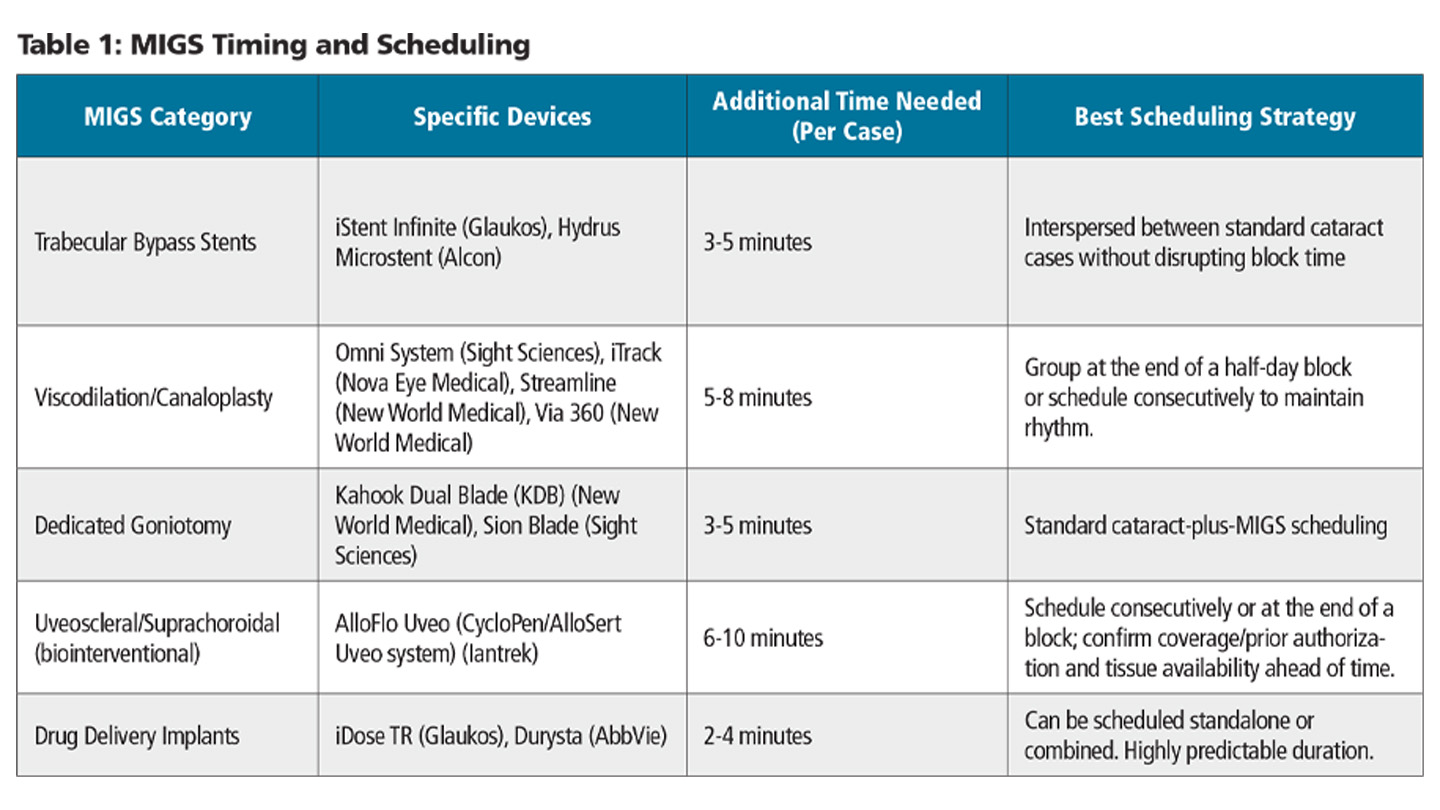
Practical Scheduling Framework
To protect block time, I recommend a simple, tiered scheduling approach based on which mechanism you’re adding. Table 1 provides a practical time guide that works well for most ASCs once the team is trained.
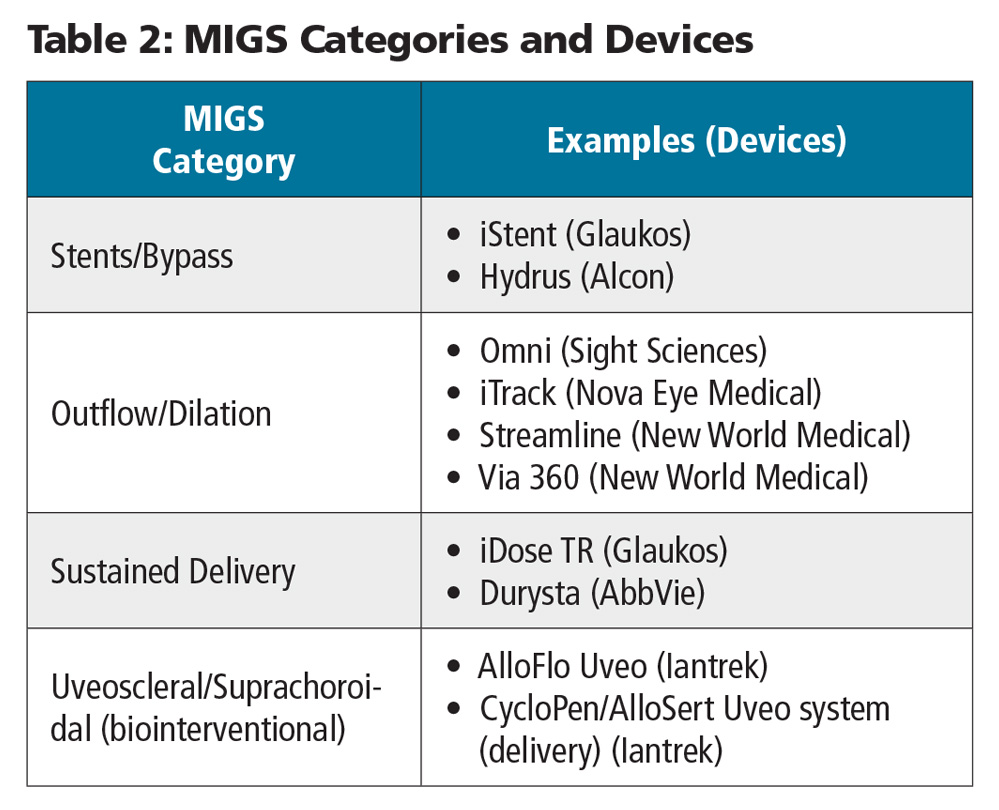
Technology Profiles: The 2026 MIGS Armamentarium
The MIGS landscape is best thought of by mechanism. Each category carries different OR demands, different cost profiles, and different “fit” within an ASC strategy (Table 2).
Trabecular Bypass Stents
iStent Infinite
The iStent Infinite (Glaukos) delivers 3 heparin-coated titanium microbypass stents via a single injector. It is US Food and Drug Administration (FDA)-cleared for adult patients with refractory primary open-angle glaucoma (POAG) who have failed prior medical and/or surgical therapy. From a documentation standpoint, I am careful to capture disease severity, medication burden, and prior interventions (eg, selective laser trabeculoplasty and prior glaucoma procedures) to align with payer expectations.
- ASC considerations: Implant-only workflow keeps the room simple, no viscodilation and no special tray turnover. When I’m combining cataract and MIGS, I typically do the angle work upfront. This reduces the chance of opening extra ophthalmic viscosurgical device (OVD), and it gives time for hemostasis before we finish the case, which can help minimize postoperative hyphema.
Hydrus Microstent
The Hydrus Microstent (Alcon) is an 8-mm nitinol scaffold placed within Schlemm’s canal. It bypasses the trabecular meshwork while dilating and scaffolding the canal across roughly 3 clock hours.
- ASC considerations: This integrates cleanly into routine cataract workflow with a single-use injector. The key is consistent angle visualization and disciplined positioning. An implant that is even slightly malpositioned can create avoidable downstream issues. Long term, I counsel surgeons to watch for peripheral anterior synechiae that can form over the outflow segment.
Viscodilation and Canaloplasty With or Without Goniotomy or Trabeculotomy
These technologies focus on mechanically restoring the eye’s natural drainage system by dilating Schlemm’s canal and collector channels.
Omni System
The Omni System (Sight Sciences) allows a combined canaloplasty and goniotomy using a single handheld device. It involves microcatheterization of Schlemm’s canal (180° or 360°), followed by viscodilation and/or unroofing of the trabecular meshwork. I like that it can be performed through the primary incision, which may reduce the need for additional paracenteses. A limitation is that the device is not directly visualized as it tracks; in tight angles or when resistance is encountered, false passage into collector channels or breakthrough into the anterior chamber can occur.
- ASC considerations: The Omni system requires a manual infusion of viscoelastic. Administrators should account for the cost of the device and the associated high-viscosity OVD when calculating supply expenses.
iTrack
The iTrack microcatheter (Nova Eye Medical) is a workhorse for ab-interno canaloplasty. The illuminated tip gives true 360° positional feedback as the catheter advances around Schlemm’s canal, followed by pressurized viscodilation. To optimize access and reduce catheter kinking, I typically create 2 additional paracenteses oriented toward the 3 and 9 o’clock positions. One practical advantage is the ability to deliver viscoelastic more uniformly; the shearing effect temporarily modifies the viscosity of the OVD, which allows for effective dilation of the collector channels as well.
- ASC considerations: The device requires a dedicated console for the light source and viscoelastic delivery, which Nova Eye provides to the ASC. The ASC must manage the small footprint of this capital equipment in the OR.
Via 360 and Streamline
The Via 360 and Streamline Surgical Systems (New World Medical) are designed to perform canaloplasty combined with precise microgoniotomies. They deliver viscodilation in metered, controlled doses directly into the canal. Surgeons must carefully visualize the device to ensure it does not accidentally go down a collector channel. In addition, surgeons need to get comfortable with maintaining forward pressure while delivering viscoelastic, which can be a challenge.
- ASC considerations: These are fully single-use, disposable surgical handpieces. They do not require a capital equipment footprint, which simplifies prep and setup times for technical staff.
Drug Delivery Devices
Sustained-release drug delivery systems address patient compliance issues by providing targeted, long-term medication directly within the anterior segment.
iDose TR
The iDose TR travoprost intracameral implant (Glaukos) is anchored through trabecular meshwork to the back wall of Schlemm’s canal and delivers sustained intraocular pressure (IOP) lowering for roughly 24 to 36 months. For cataract surgeons expanding into interventional glaucoma, this can be an approachable on-ramp to angle-based work. A key consideration is that iDose TR can also be combined with other MIGS at the same sitting. One important counseling point: iris pigmentation changes can occur and may be clinically meaningful. Surgeons and surgery counselors must set that expectation preoperatively with patients.
- ASC considerations: The iDose TR requires an efficient inventory management strategy. ASCs typically acquire the device via the buy-and-bill process or through a specialty pharmacy.
Durysta
Durysta (AbbVie) is a biodegradable intracameral implant containing 10 mcg of bimatoprost. It settles in the inferior anterior chamber angle and releases the medication over several months as the implant dissolves.
- ASC considerations: Because Durysta does not require visual confirmation through a goniolens for placement, it can be administered quickly at the end of a procedure or in an office-based procedure room.
Dedicated Goniotomy Devices
Dedicated goniotomy devices excise or incise trabecular meshwork to create a direct pathway into Schlemm’s canal. From a reimbursement standpoint, many payers expect documentation that a dedicated goniotomy device was used, therefore your coding and operative note should be aligned with current payer policy.
Kahook Dual Blade
The Kahook Dual Blade (KDB; New World Medical) uses a dual-blade design to create a controlled excision of trabecular meshwork. This is another strong entry point for surgeons learning angle-based surgery, and it’s titratable. Treat the arc length that matches the patient’s disease and risk tolerance. As with any trabecular procedure, be prepared for hyphema—proactive counseling and a consistent postoperative plan matter.
- ASC considerations: As a single-use manual instrument, the KDB eliminates sterilization cycles. It is easily scheduled and can be completed in just a few minutes.
Sion Surgical Instrument
The Sion blade (Sight Sciences) is a single-use surgical instrument designed to excise trabecular meshwork tissue with smooth, continuous movements.
- ASC considerations: Like the KDB, it has a low learning curve and a minimal operational footprint in the OR.
New Biointerventional Device
We are also seeing a return to the suprachoroidal space with the emergence of biointerventional approaches, most notably, AlloFlo Uveo (Iantrek). Conceptually, this shifts the conversation from permanent synthetic hardware toward leveraging the eye’s uveoscleral outflow pathway with a biologic spacer strategy.
- Biotissue advantage: AlloFlo is a hardware-free, allogeneic biospacer crafted from minimally manipulated donor scleral tissue.
- Uveoscleral target: Rather than focusing on trabecular bypass, the goal is to access the suprachoroidal space and promote pressure-independent outflow through the uveoscleral pathway.
- Procedure: The CycloPen System (Iantrek) creates a controlled cyclodialysis cleft, followed by the AlloSert Uveo (Iantrek) handpiece to position 500 µm × 5 mm biospacers intended to help maintain long-term patency. Typically, between 1 and 3 spacers are placed to maintain 1 or 2 clefts.
- Clinical signal:In the CREST study, reported outcomes included a 42% mean IOP reduction at 12 months, with low rates of issues such as iris inflammation or implant migration consistent with a bio-integrating approach.
Emerging Laser Technologies: Elios Excimer Laser Trabeculostomy
The Elios system (Bausch + Lomb) is in development as an implant-free technology designed to treat elevated IOP in open-angle glaucoma. The system uses an excimer laser via a micro-probe to create 10 microchannels in the trabecular meshwork. This enhances aqueous outflow without leaving a permanent implant behind. The system is currently under final review with the US Food and Drug Administration.
- ASC considerations: Because the system relies on an excimer laser console, storage space needs to be considered, especially if multiple devices are required for a busy ASC with multiple surgeons operating simultaneously. Operationally, it requires the laser probe to be integrated into the surgical field similar to the iTrack device.
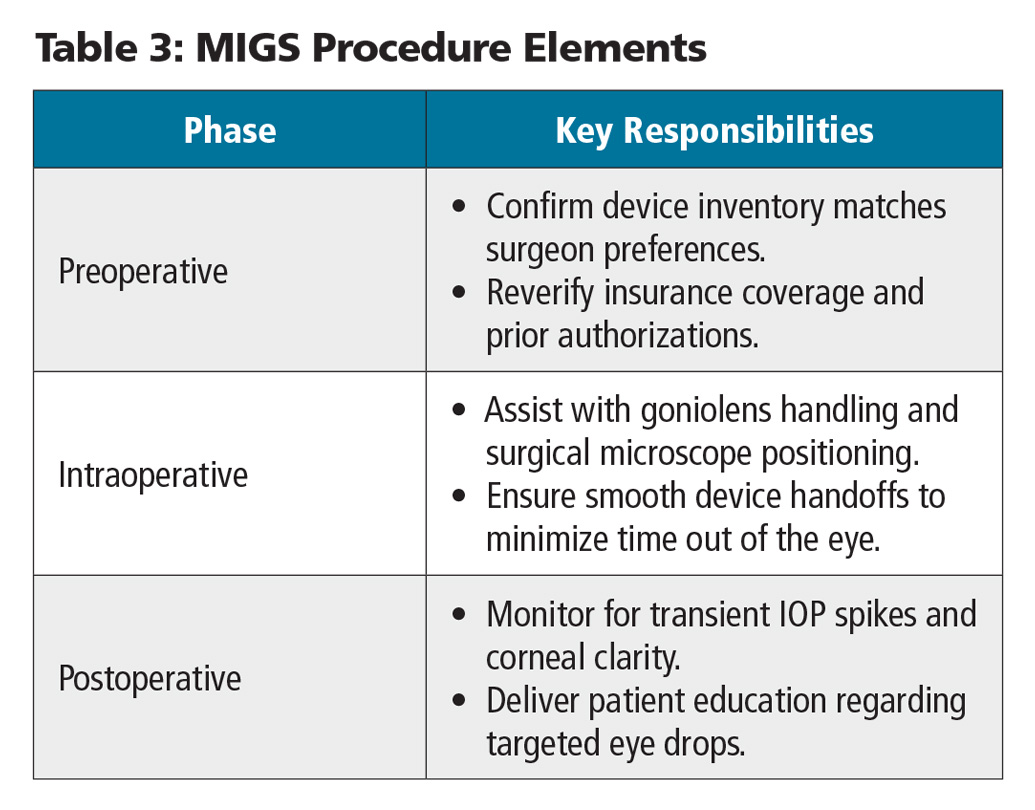
Operational Execution in the OR: Roles and Responsibilities
Executing a high-efficiency MIGS program requires a well-trained surgical team. Cross-training staff on these specific procedures ensures that scheduling blocks run smoothly (Table 3).
The Patient Experience
As we continue to grow the interventional glaucoma marketplace, patients should understand that adding a MIGS procedure to their cataract surgery does not prolong their recovery time. They should expect clear vision soon after surgery, along with the long-term benefit of potentially reducing their daily glaucoma drop burden. In our practice, we are proactive with explaining not only the drop burden to patients, but also the damage caused to the ocular surface (dry eye disease, meibomian gland dysfunction, limbal stem cell deficiency) and potentially to the trabecular meshwork itself secondary to toxic effects of preservatives and drugs themselves.
Preoperative Nursing Staff
- Verification: Confirm the specific device requested matches the patient’s diagnosis code (eg, matching mild/moderate vs severe/refractory POAG).
- Inventory control:Ensure the correct single-use injectors or blades are readily available in the OR.
Intraoperative Scrub Technicians and Circulating Nurses
- Goniolens management: The scrub technician must have the goniolens sterile and ready for use.
- Viscoelastic handling: If using systems like the Omni or iTrack, the scrub technician must pre-load the designated viscoelastic and have the handpiece primed.
- Microscope ergonomics: The circulating nurse must be ready to assist with tilting the microscope and the patient's head to maintain a direct view of the anterior chamber angle.
Postoperative Recovery (PACU) Nurses
- Patient education: Instruct the patient on any modifications to their eyedrop regimen, such as tapering off specific glaucoma medications or adjusting their steroid regimen.
The Financial Value Proposition
For the ASC owner and administrator, adding MIGS procedures must make financial sense. The economic viability of these cases depends on precise coding, favorable commercial contracts, and clear management of device-intensive surgical costs.
Medicare and Commercial Reimbursement Overview
Under the 2026 CMS Ambulatory Surgical Center Payment System updates, several MIGS procedures fall within the device-intensive category. This classification helps align facility compensation with the high acquisition costs of these implants.
- ASC conversion factor: The 2026 ASC conversion factor is $56.322, reflecting a 2.6% payment increase for facilities meeting quality reporting metrics.
- The Multiple Procedure Reduction Rule: When a MIGS procedure is billed in conjunction with cataract extraction, Medicare pays 100% of the highest-paying procedure (typically the MIGS code) and 50% of the second procedure (the cataract code).
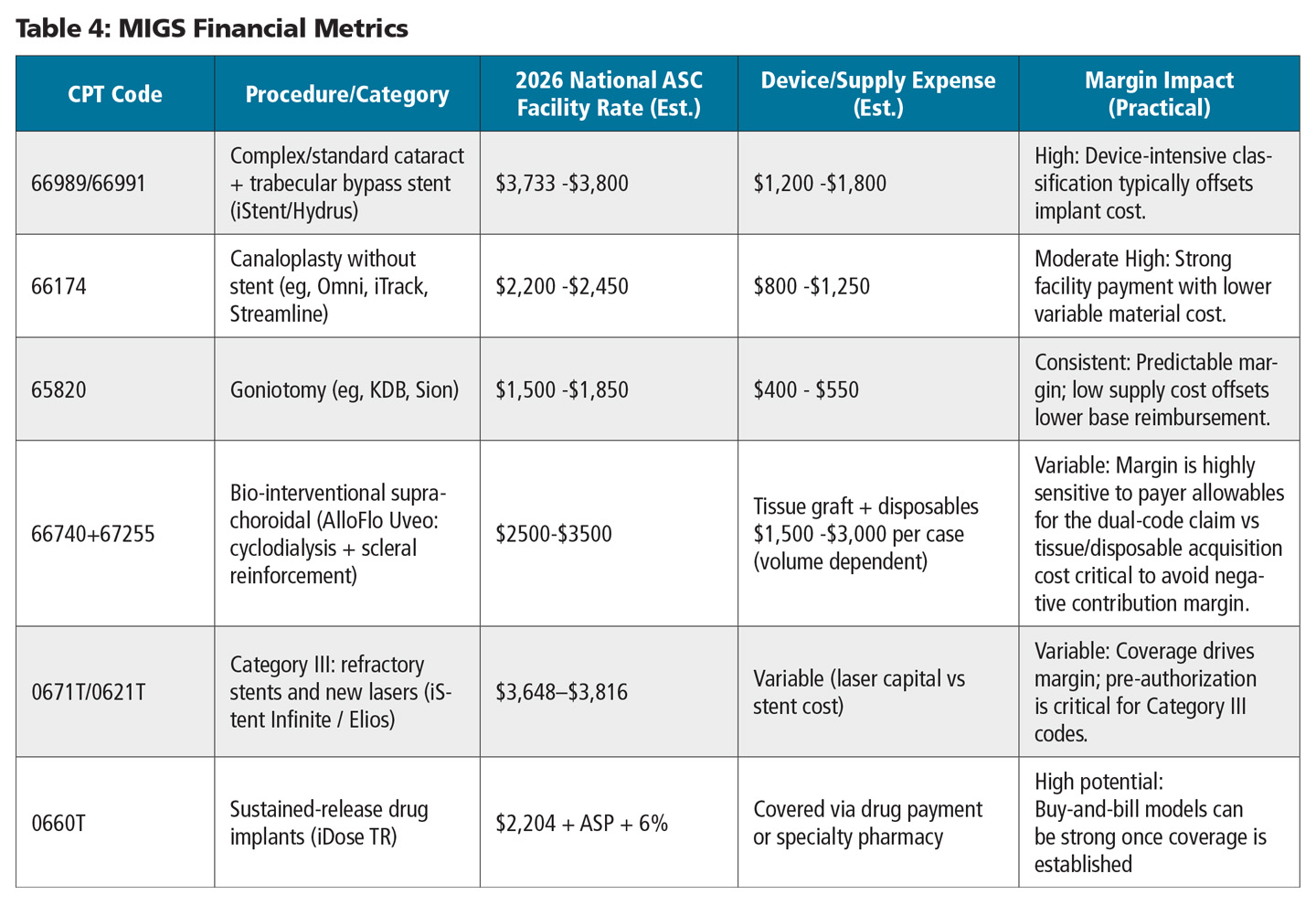
2026 Financial Metrics by Procedure Class
The financial success of a MIGS program comes down to net margin: the difference between facility payment and the true, all-in device/supply cost. A second (often overlooked) variable is surgeon professional fee, which can influence adoption and case mix. In practice, alignment between ASC ownership, management, and surgeons is essential (Table 4).
Strategic Financial Takeaways for Administrators
- Device-intensive optimization: Review the device-intensive status of high-cost implants before scheduling. In 2026, CMS continues to designate combined cataract-plus-stent codes as device-intensive, which prevents supply expenses from outstripping facility payments.
- Managing the supply chain: Formulary standardization is critical. Rather than stocking every available MIGS device, select 1 or 2 core options across the primary categories (eg, 1 trabecular bypass stent and 1 viscodilation device). This strategy helps the ASC leverage bulk purchasing agreements and volume tiers with manufacturers.
- Negotiating commercial carveouts: When negotiating commercial contracts, ensure that high-cost MIGS devices are not bundled into a general ophthalmic rate. Commercial payers should include a separate carveout for the implant or base their reimbursement on a percentage of the billed device charges.
- Managing prior authorizations: To minimize payment delays, ensure the patient's record matches the specific FDA-approved indication for each procedure. For example, some commercial payers limit goniotomies and trabeculotomies to certain diagnoses. Verifying prior authorizations in advance protects the ASC from costly claim denials.
Strategic Insights and Data-Driven Path to ASC Growth
Success in interventional glaucoma is not just “doing the surgery.” It is building a repeatable system that scales clinically, operationally, and financially. In my experience, the ASCs that win in 2026 are deliberately data driven about device selection, workflow, and payer strategy.
- Standardize your formulary: You don’t need every device. Pick a core trabecular bypass option, a canal-based dilation option, and a uveoscleral/suprachoroidal option—then build volume and negotiate from strength.
- Protect margin with commercial carve-outs: Don’t allow high-cost MIGS (including biologic and drug-delivery platforms) to be bundled into a generic ophthalmic rate. If you can’t carve out, you’ll eventually ration clinically appropriate care.
- Elevate patient education: I frame MIGS as a long-term ocular-surface and quality-of-life decision—not “one more procedure.” Patients increasingly understand the burden of chronic drops and preservatives.
- Train the room, not just the surgeon: Standardize the angle setup, gonioprism handling, microscope/head tilt, and device handoffs so MIGS is time neutral on cataract days.
- Schedule with intention: Use tiered templates and cluster longer-mechanism cases when needed to protect throughput and staff rhythm.
Done well, MIGS expands options for patients, improves predictability for the OR, and builds a durable glaucoma service line that strengthens the ASC. The centers that succeed are the ones that treat MIGS as a program—mechanism-based selection, disciplined workflow, and payer alignment—not a collection of devices. OASC
